Finasteride is widely prescribed for male pattern hair loss and benign prostate enlargement. For many men, it slows progression of androgenetic alopecia and helps preserve scalp coverage over time. But alongside its growing use, concerns about mental health side effects have received increasing medical attention.
One question appears repeatedly in clinics, online discussions, and regulatory reviews. Can finasteride cause depression?
The most medically accurate answer is that mood related side effects have been reported, recognised by regulators, and taken seriously by researchers. However, the relationship is complex, and current evidence does not prove that every depressive symptom experienced during finasteride use is directly caused by the medication itself.
Some men report no psychological changes at all. Others describe low mood, anxiety, emotional blunting, or depressive symptoms that began during treatment. A smaller group report symptoms persisting after discontinuation.
Understanding what is known, what remains uncertain, and where internet discussions sometimes oversimplify the issue is important for balanced decision making.
How finasteride works
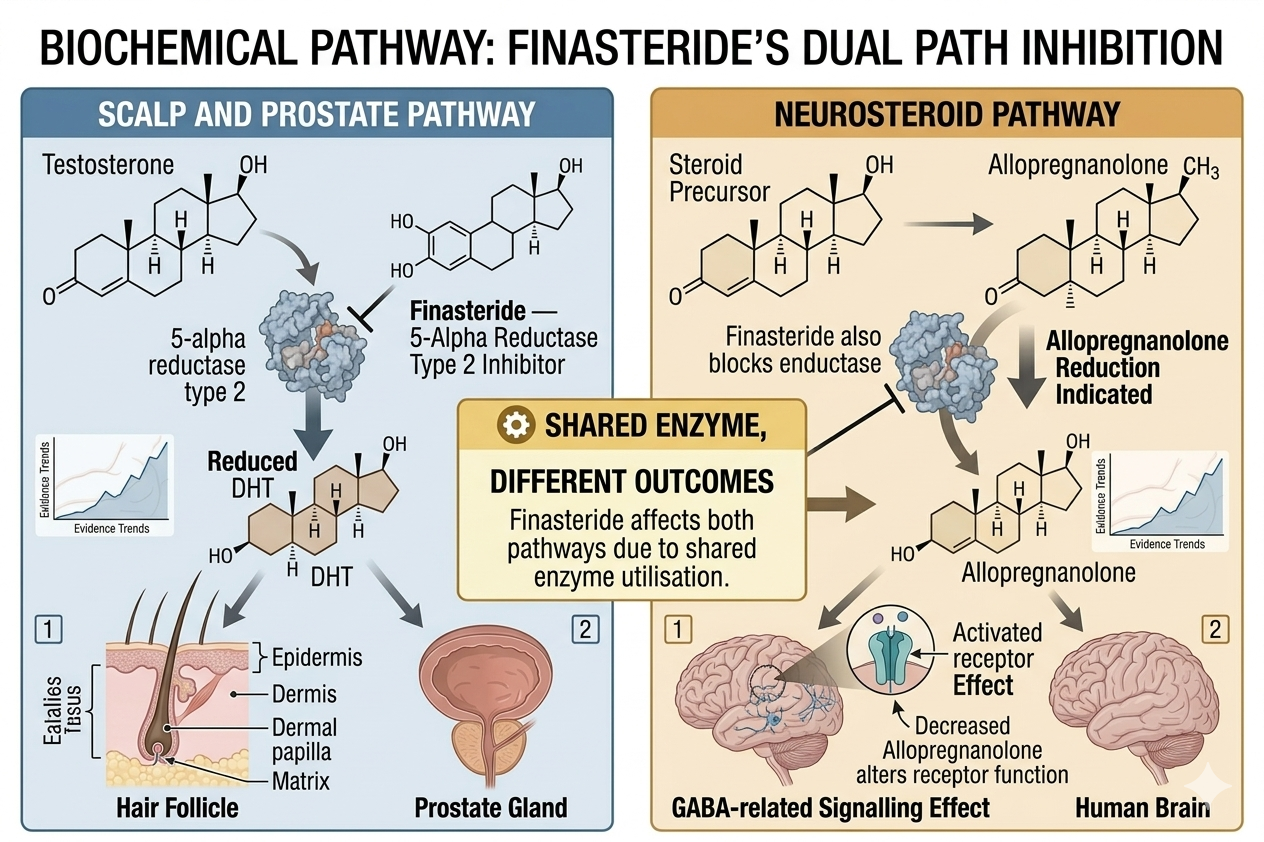
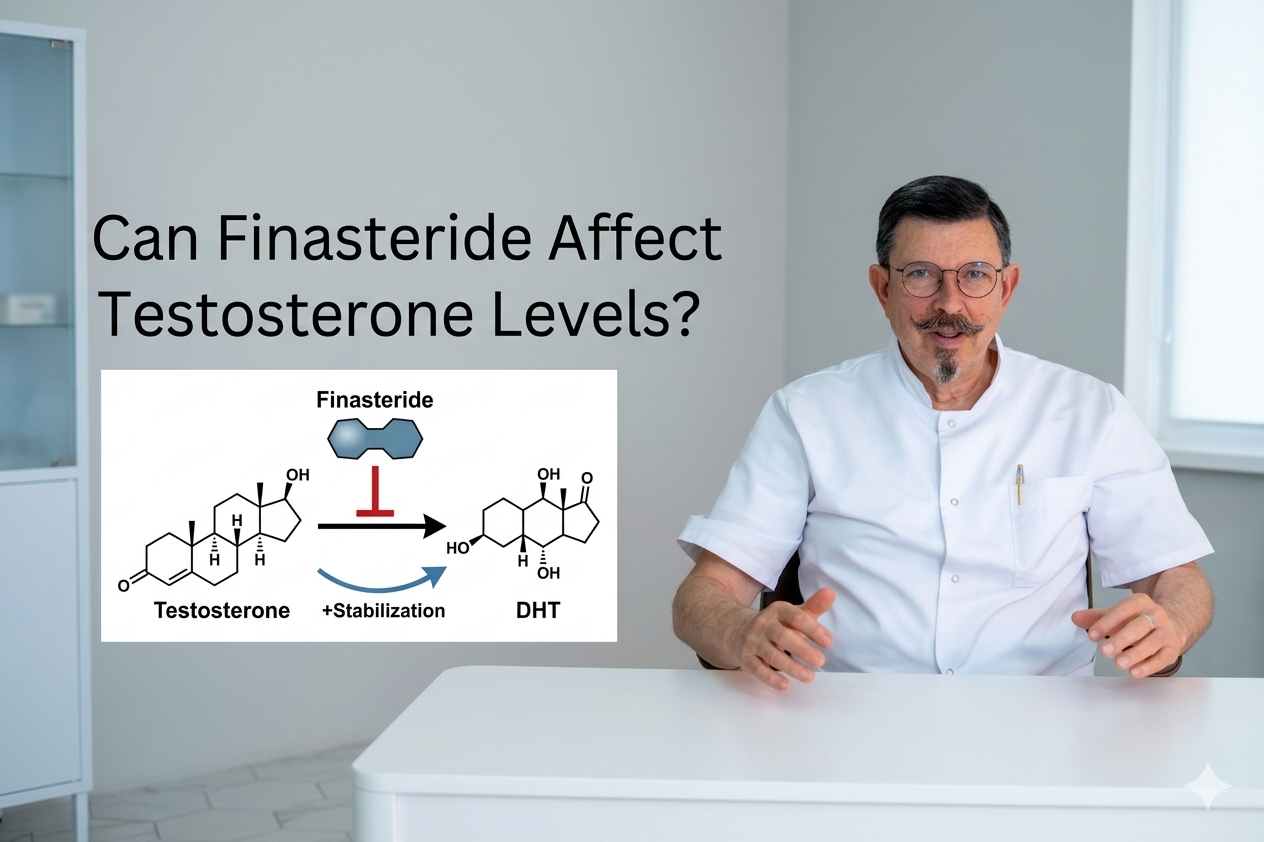
Finasteride blocks the enzyme 5 alpha reductase type 2. This enzyme converts testosterone into dihydrotestosterone, or DHT.
DHT plays a major role in androgenetic alopecia. By lowering DHT levels, finasteride can reduce progressive miniaturisation of scalp hair follicles.
However, 5 alpha reductase enzymes are not limited to the scalp or prostate. They are also involved in pathways related to neurosteroids, which are hormone like substances active in the brain and nervous system.
This is one reason researchers have explored whether finasteride could influence mood or mental wellbeing in certain individuals.
Are depression and mood changes recognised side effects?
Yes.
Mood related side effects have been included in regulatory safety reviews involving finasteride.
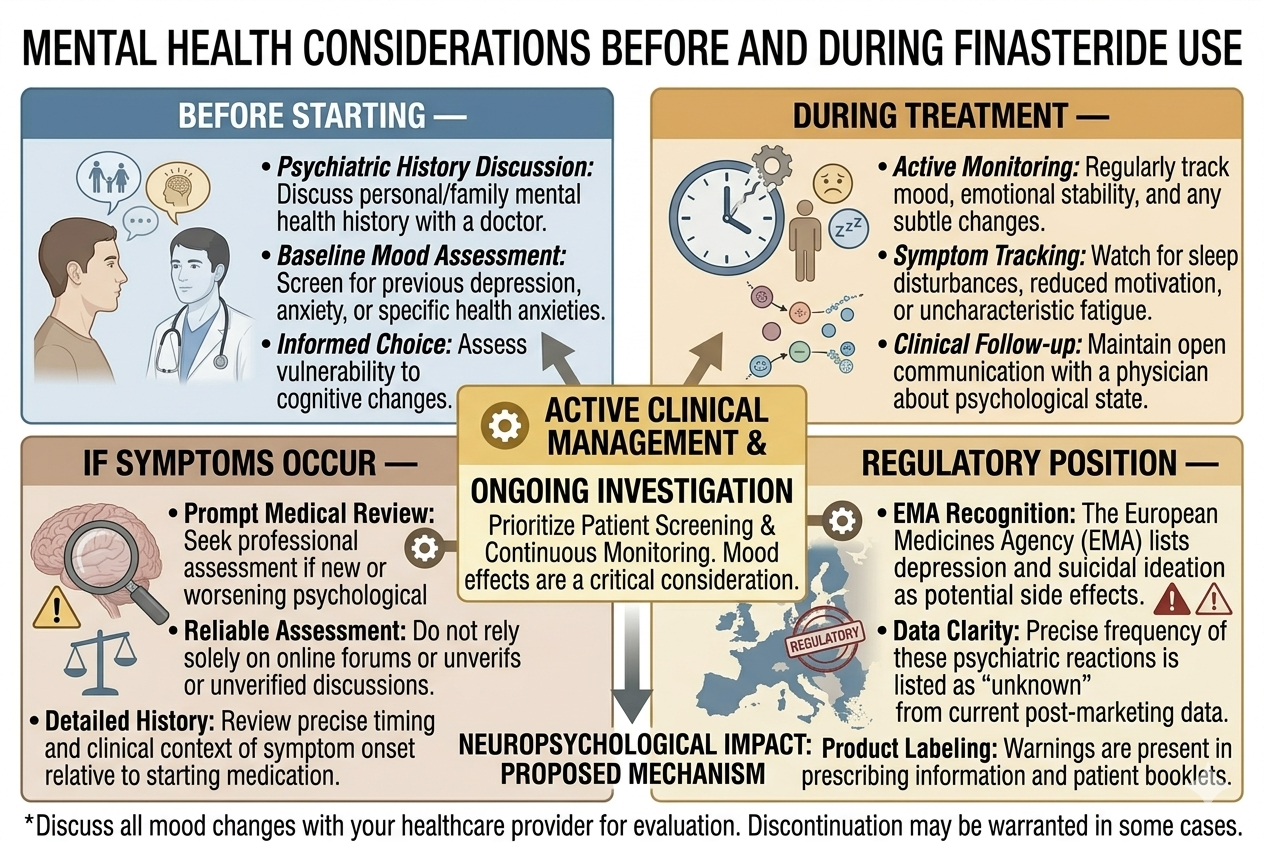
In Europe, the European Medicines Agency reviewed available safety data and confirmed suicidal ideation as a side effect of finasteride tablets, although the exact frequency could not be determined from available evidence. Patients using finasteride for hair loss are advised to seek medical advice if they experience depressed mood, depression, or suicidal thoughts.
This does not mean finasteride causes depression in most users. It means sufficient concern exists for regulators to formally acknowledge the possibility.
What symptoms have been reported?
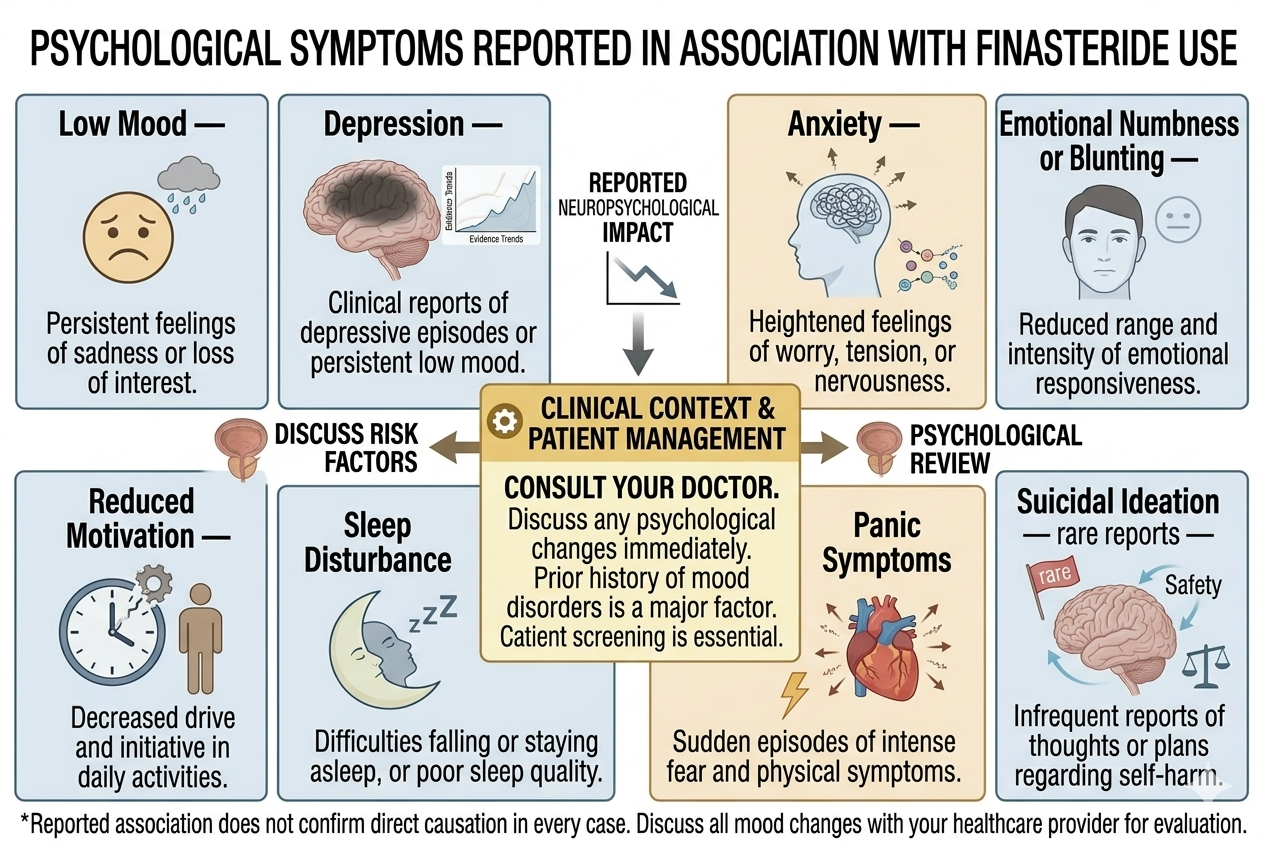
Reported psychological symptoms associated with finasteride have included:
- Low mood.
- Depression.
- Anxiety.
- Emotional numbness or blunting.
- Reduced motivation.
- Sleep disturbance.
- Panic symptoms.
- Suicidal thoughts in rare reports.
Not every report proves causation. Depression is common in the general population and can arise from many overlapping biological, psychological, and social factors.
Still, repeated reports across clinical practice and pharmacovigilance systems mean the issue cannot simply be dismissed.
Why is the evidence difficult to interpret?
This area of medicine is complicated for several reasons.
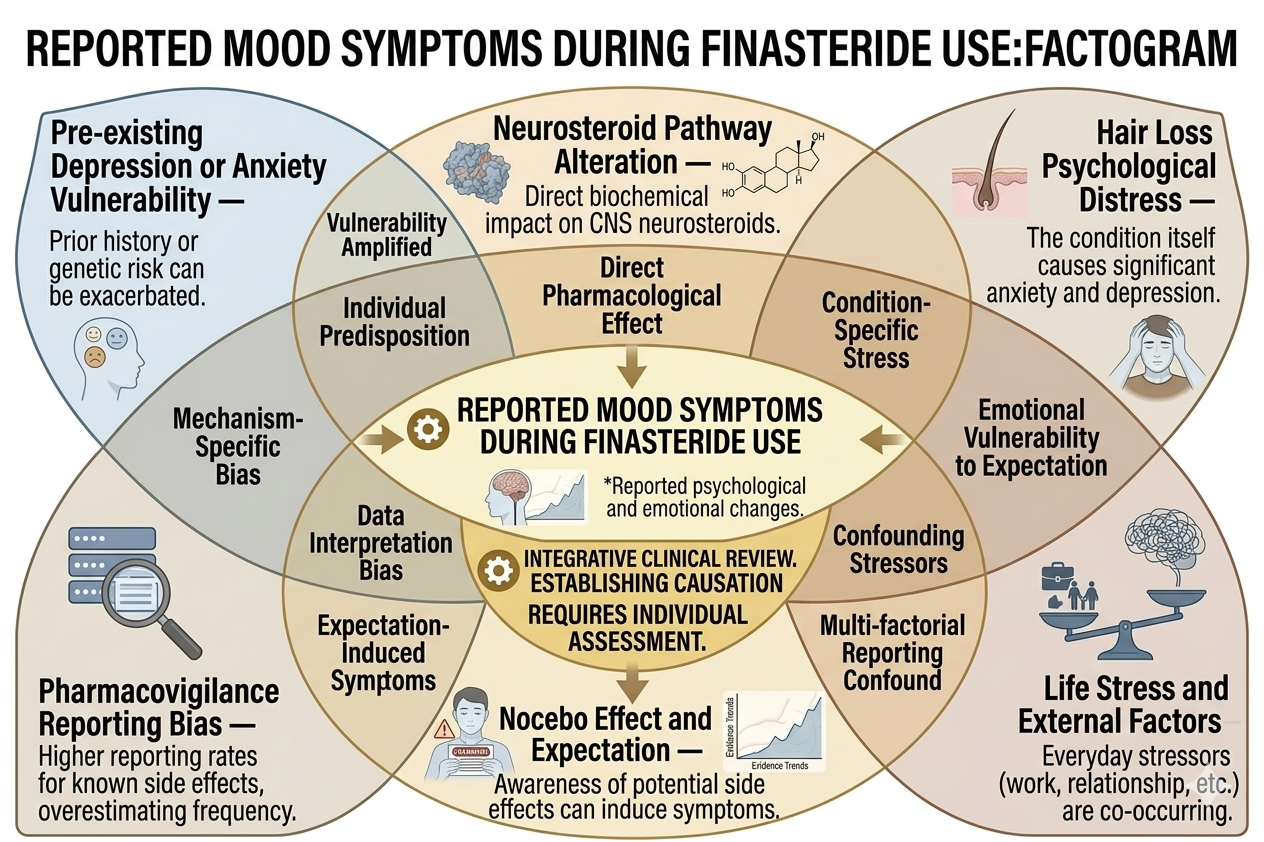
First, depression and anxiety are already common conditions, particularly in younger and middle aged adults who may also be distressed by hair loss itself.
Second, online discussions about finasteride can strongly influence expectations and symptom awareness. Fear and hypervigilance may affect how people interpret physical or emotional changes during treatment.
Third, many studies differ in quality, design, patient selection, and symptom definitions. Some rely heavily on self reporting rather than objective measures.
Finally, mental health symptoms are influenced by sleep, relationships, stress, work pressure, substance use, hormonal factors, and existing psychiatric vulnerability.
Because of this, proving direct biological causation in every individual case is difficult.
Does hair loss itself affect mental health?
Yes. This point is sometimes overlooked.
Androgenetic alopecia can affect self image, confidence, social comfort, ageing perception, and psychological wellbeing. Some men experience significant distress related to hair loss even before treatment begins.
For certain individuals, successful hair treatment may actually improve confidence and emotional wellbeing.
This creates a complicated clinical picture. A man taking finasteride may simultaneously experience psychological benefits from stabilising hair loss while also worrying about possible side effects.
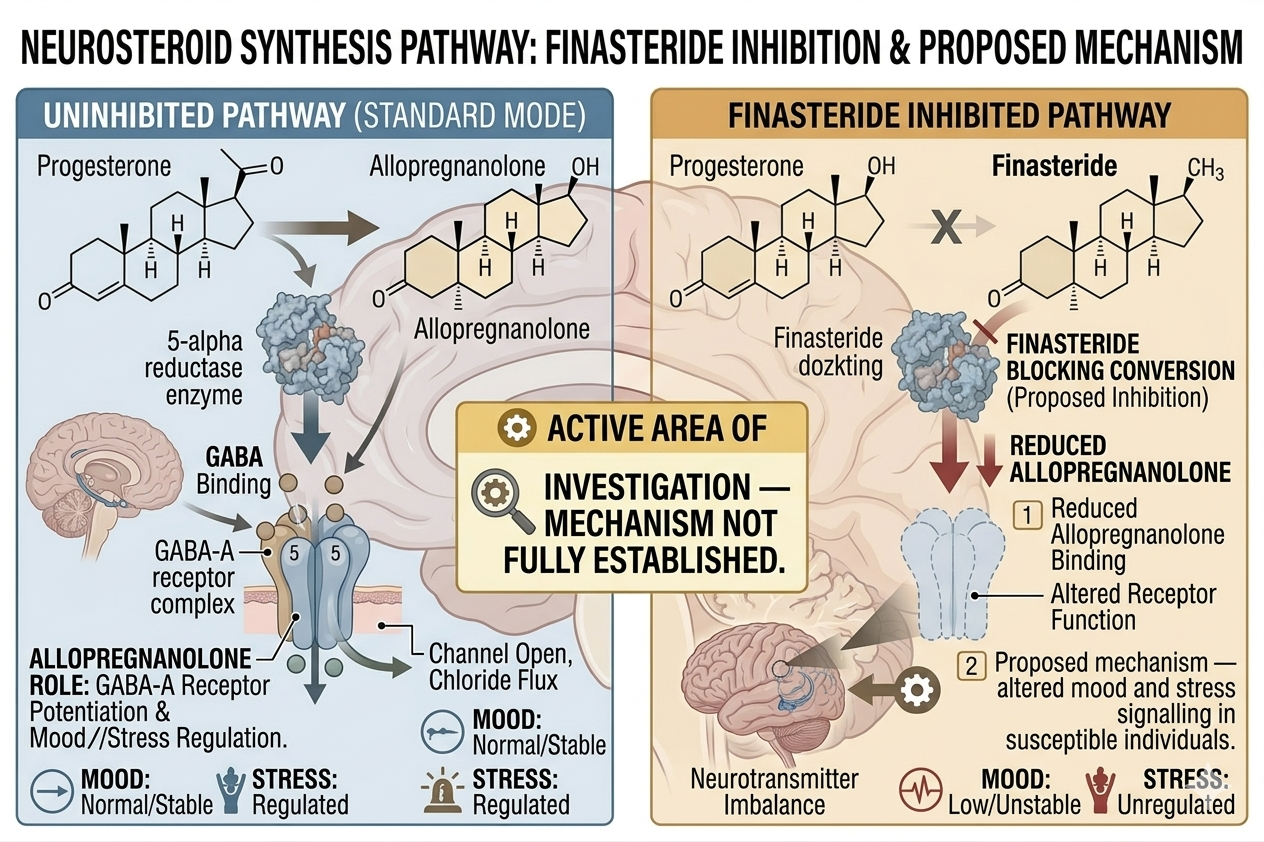
What are neurosteroids and why are they discussed?
Finasteride affects conversion pathways involved not only in DHT production but also in certain neurosteroids active within the brain.
One neurosteroid often discussed is allopregnanolone, which influences GABA related signalling involved in mood and stress regulation.
Researchers have proposed that altered neurosteroid balance could potentially contribute to mood symptoms in susceptible individuals. However, this remains an active area of research rather than a fully settled mechanism.
Not every person exposed to neurosteroid changes develops psychiatric symptoms, which suggests individual vulnerability likely matters.
Does everyone taking finasteride become depressed?
No.
Most men taking finasteride do not report severe depression. Many tolerate treatment without major psychological effects.
At the same time, absence of symptoms in most users does not invalidate the experiences of men who report mood changes during treatment.
Good medicine avoids extremes. Finasteride should neither be portrayed as universally dangerous nor as completely incapable of affecting mental health.
What about post finasteride syndrome?
Some patients report persistent sexual, neurological, and psychological symptoms after stopping finasteride. This group of symptoms is sometimes referred to as post finasteride syndrome.
Reported psychiatric symptoms may include ongoing depression, anxiety, cognitive complaints, and emotional blunting.
The condition remains controversial in medicine because no definitive biological marker or universally accepted diagnostic criteria currently exist. Some researchers believe persistent effects may occur in vulnerable individuals. Others argue evidence is limited by selection bias, nocebo effects, inconsistent methodology, and overlapping psychiatric conditions.
The debate remains ongoing.
Can anxiety about finasteride contribute to symptoms?
Possibly.
The nocebo effect refers to symptoms influenced by negative expectations surrounding treatment. This effect is real and well documented across medicine.
A patient reading frightening online accounts may become intensely focused on mood, sexual function, or bodily sensations. Anxiety itself can produce fatigue, sleep disturbance, low libido, reduced concentration, and depressive symptoms.
This does not mean all reported symptoms are imaginary. It means psychological and biological processes can interact in complicated ways.
Should men with previous depression avoid finasteride?
Not necessarily, but caution is sensible.
Men with a history of depression, anxiety disorders, panic attacks, obsessive health anxiety, or previous psychiatric illness may benefit from more careful discussion before starting treatment.
For some, finasteride may still be appropriate. For others, the psychological risk may outweigh cosmetic benefits.
Individual history matters more than internet generalisations.
What should men do if mood changes occur?
Mood symptoms during finasteride treatment should be taken seriously.
A patient experiencing depression, emotional blunting, worsening anxiety, or suicidal thoughts should seek medical assessment rather than relying solely on online discussions.
A doctor may review:
- Timing of symptoms.
- Medication history.
- Psychiatric background.
- Sleep patterns.
- Stress levels.
- Alcohol or substance use.
- Physical health factors.
- Potential benefit of discontinuation.
In some cases, stopping finasteride may be appropriate. In others, symptoms may relate more strongly to unrelated psychiatric or life factors.
Careful clinical evaluation matters.
Is topical finasteride safer for mental health?
Topical finasteride may produce lower systemic exposure compared with oral tablets, but absorption into the bloodstream still occurs.
Long term evidence specifically comparing psychiatric risk between topical and oral formulations remains limited.
Topical treatment should not automatically be assumed free from systemic effects.
In conclusion
Current evidence suggests finasteride can be associated with mood related side effects in some individuals, and regulators now formally recognise depression and suicidal ideation as potential risks. At the same time, most users do not develop severe psychiatric symptoms, and the exact biological mechanisms remain incompletely understood.
The relationship between finasteride and mental health is likely influenced by multiple factors including neurosteroid pathways, psychological vulnerability, stress, expectations, and individual biology.
For men considering treatment, balanced information matters more than fear based internet narratives or dismissive reassurance. Finasteride remains an evidence based treatment for androgenetic alopecia, but mental wellbeing should always be considered part of responsible prescribing and ongoing monitoring.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.
Add Comment