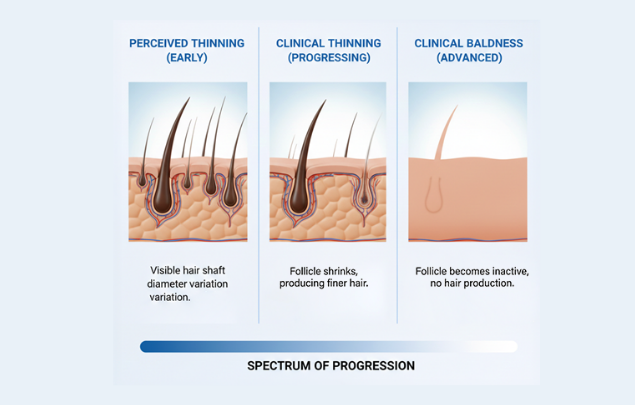
Hair thinning and baldness are often used interchangeably, but clinically, they are not the same.
Hair thinning is a description of what someone notices — a perceived change in density, volume, or hair shaft thickness. Baldness, by contrast, refers to a more advanced endpoint where specific follicles stop producing visible hair in certain scalp areas.
This distinction is important because the same perceived change can be caused by very different processes, with very different outcomes. Some causes of thinning are temporary and recover. Some stabilize. And some represent an early stage of progressive hair loss.
Hair thinning is a sign, not a diagnosis.
Whether it leads to baldness depends on the underlying process causing it — not simply on the fact that thinning is noticed.
Common situations where people first notice hair thinning
- Hair feels lighter, flatter, or harder to style
- Scalp becomes more visible under bright light or when hair is wet
- A widening part or reduced volume at the temples or crown
- Increased awareness of hair fall, even if shedding is within normal limits
These observations are common. However, they do not determine outcome on their own. The same appearance can reflect anything from temporary cycle disruption to early miniaturization.
Why identifying the cause matters
Hair thinning is often noticed before the pattern is obvious. At early stages, changes can be subtle — which is why people ask:
- “Is this the beginning of hair loss?”
- “Should I be worried?”
- “Do I need treatment already?”
At this stage, the correct approach is not to assume the worst, and it is not to treat the perception alone. The goal is to identify what is causing the thinning and whether it is stable, temporary, or progressive.
A structured assessment — using clear images, pattern review, and clinical interpretation — can often clarify stage and likely mechanism, particularly in early cases. When uncertainty remains, documentation over time can further confirm whether change is occurring.
What Doctors Mean by “Hair Thinning”
In medical practice, the term hair thinning is descriptive, not diagnostic.
It reflects how a change in hair appearance is perceived — typically a reduction in volume, density, or hair shaft thickness — but it does not define the biological process responsible for that change.
Clinically, diagnosis does not focus on “thinning” itself. It focuses on what is causing the appearance of thinning, because very different mechanisms can produce the same visual impression.
Different processes that can appear as thinning
| What’s happening | What it means clinically | Does it lead to baldness? |
|---|---|---|
| Increased shedding | More hairs shift into the resting phase at the same time | Usually no |
| Reduced active density | Fewer hairs growing simultaneously in an area | Sometimes |
| Follicle miniaturization | Hairs regrow progressively thinner with each cycle | Yes, if ongoing |
Although these situations can look similar when someone examines their hair, their implications are very different.
Shedding is not a diagnosis
Many people equate hair thinning with hair fall. Clinically, this is not always accurate.
Shedding reflects a change in the hair growth cycle, not follicle damage. It can occur after:
- Physical or emotional stress
- Illness or surgery
- Hormonal changes
- Nutritional imbalance
In these cases, follicles remain structurally intact and capable of producing normal hair. The perception of thinning can be pronounced, even though the underlying condition is temporary.
Reduced density does not always indicate progression
Hair density refers to how many hairs are actively growing in a given scalp area at a given time. Density can fluctuate naturally, and a mild reduction does not automatically indicate disease.
In early or borderline cases, density may stabilize without progressing — particularly when hair shaft diameter remains consistent and follicle structure is preserved.
This is why classification depends on mechanism, not appearance alone.
Miniaturization is the defining distinction
Baldness develops only when hair follicles progressively miniaturize and produce thinner hairs with each growth cycle.
This process is characteristic of androgenetic alopecia. It develops gradually and often begins before bald areas are visible. At early stages, miniaturization may not be obvious without structured visual assessment and clinical interpretation.
Why precise language matters
Referring to thinning as if it were a condition can be misleading.
It can cause unnecessary worry when hair is likely to recover — or false reassurance when a progressive process is beginning.
For this reason, clinical assessment focuses on:
- The mechanism causing the appearance of thinning
- The pattern across the scalp
- Whether change is stable or evolving
Only after these are clarified can the question “does hair thinning lead to baldness?” be answered meaningfully for an individual.
How Hair Thinning Can Progress to Baldness
Hair thinning leads to baldness only under specific biological conditions.
The determining factor is not how thin the hair appears, but whether the process causing that appearance involves progressive follicle miniaturization.
Thinning itself does not progress. The underlying condition may.
The mechanism that links thinning to permanent hair loss
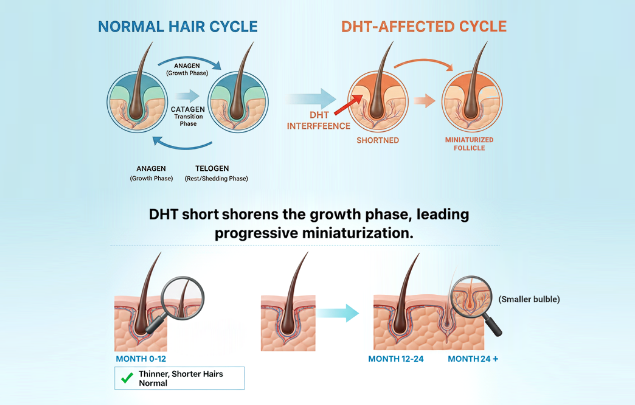
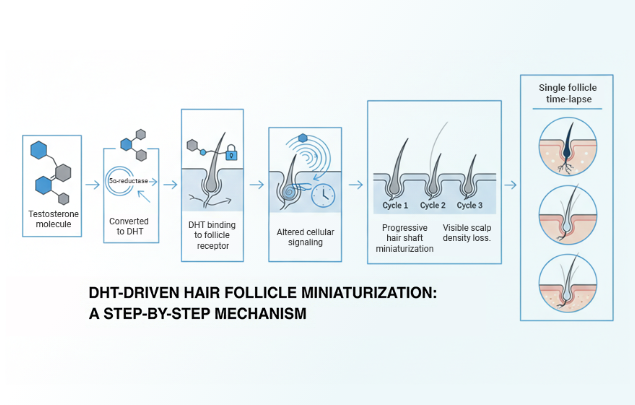
In androgenetic alopecia, certain hair follicles are genetically sensitive to androgens — particularly dihydrotestosterone (DHT).
When this sensitivity is present, a gradual process unfolds:
- Testosterone is converted into DHT by enzymes in the scalp
- DHT binds to receptors in susceptible follicles
- Growth signals within the follicle change
- Each growth cycle produces a shorter, finer hair
- Over time, visible density is reduced in affected areas
This explains why thinning is often noticed before baldness appears, and why early changes can feel ambiguous despite an active process already being present.
Why thinning alone does not determine outcome
Hair thinning leads to baldness only when follicle miniaturization is ongoing.
If follicles remain structurally intact, the appearance of thinning may stabilize or reverse.
Many people experience thinning without this mechanism ever becoming active. In those cases, hair does not continue to deteriorate indefinitely.
Genetics influence susceptibility, not certainty
Genetic predisposition determines whether follicles are sensitive to DHT.
However, it does not determine:
- When thinning becomes noticeable
- How quickly progression occurs
- Whether progression continues beyond early stages
This variability explains why some individuals thin early and never go bald, while others show gradual change over many years.
The role of visual assessment at early stages
At early stages, progression is often localized and subtle, not diffuse or dramatic.
When visual information is structured — reviewed for pattern, distribution, and hair shaft variation — clinicians can often determine whether miniaturization is present and assign an early stage.
In some cases, follow-up comparison over time is helpful. In others, a single structured visual assessment is sufficient to classify the process and guide next steps.
What this means at early stages
At early stages, thinning may reflect:
- A temporary change
- A stable, non-progressive pattern
- Or early androgen-driven miniaturization
The role of evaluation is not to predict baldness, but to identify which process is responsible so that monitoring or treatment decisions are appropriate.
Only after this distinction is made does it make sense to discuss reassurance, observation, or intervention.
Causes of Hair Thinning That Do Not Lead to Baldness
Not all perceived hair thinning reflects a progressive hair loss condition.
In many cases, the appearance of thinning results from temporary or reversible changes in the hair growth cycle, rather than from follicle damage or miniaturization.
In these situations, the perception of thinning improves once the underlying cause resolves.
Common causes where thinning reflects cycle disruption, not follicle loss
Temporary cycle disruption
- Physical or emotional stress
- Acute illness or surgery
- Significant weight change
- Post-partum hormonal shifts
Hormonal or metabolic influences
- Thyroid imbalance
- Iron deficiency
- Nutritional insufficiency
Medication-related effects
- Certain hormonal therapies
- Changes to long-term systemic medications
In all of these cases, hair follicles remain structurally intact. The change is driven by timing — more hairs entering a resting phase at once — not by progressive follicle shrinkage.
What non-progressive thinning looks like clinically
When thinning reflects a non-progressive process, clinicians typically observe:
- Diffuse distribution rather than focal or patterned loss
- Symmetry across the scalp
- Preserved hair shaft diameter
- Stability over time rather than directional change
These features distinguish temporary or stable causes from androgen-driven hair loss.
Recovery follows the hair cycle, not the calendar
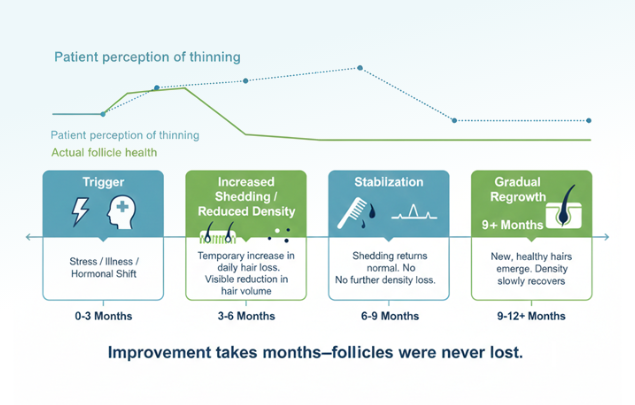
Because hair grows in cycles, visible improvement is slow. Even after the underlying cause resolves, it may take several months before density and volume normalize. During this period, the appearance of thinning can persist despite healthy follicles.
Why reassurance is sometimes the correct clinical outcome
When follicles are intact and thinning is stable, treatment does not improve outcomes.
In these cases, reassurance, observation, and time are appropriate medical responses. Intervening without evidence of progression offers no benefit and may create unnecessary concern.
When non-progressive thinning is mistaken for hair loss
Temporary or diffuse thinning is often mistaken for early baldness because:
- Scalp visibility changes with lighting and styling
- Hair volume affects how thinning is perceived
- Shedding draws attention even when follicles are healthy
Without structured assessment, these changes are easy to misinterpret.
The purpose of evaluation in these cases
Evaluation is often used to exclude progressive hair loss, not to confirm it.
When assessment shows preserved follicles and stability, the appropriate conclusion is not treatment — it is reassurance and monitoring.
When Hair Thinning Becomes Progressive Hair Loss
Up to this point, we have discussed forms of hair thinning that do not lead to baldness.
The next step is to explain when thinning represents an active, progressive process , rather than a temporary or stable change.
This distinction is central to determining whether intervention is appropriate.
What defines progressive hair loss clinically
Hair thinning becomes progressive when it is driven by ongoing follicle miniaturization.
In this situation, hair follicles remain alive but gradually produce shorter, finer, and weaker hairs with each growth cycle.
Over time, this process can result in visible scalp exposure and, eventually, baldness if left untreated.
Hallmarks of progressive thinning
Clinicians look for several consistent features:
- Patterned distribution
- Temples, frontal hairline, mid-scalp, or crown
- Gradual worsening over time
- Changes measured in months to years, not weeks
- Reduction in hair shaft diameter
- New hairs appear finer than older hairs
- Loss of density in specific zones
- Rather than uniform thinning across the scalp
These features distinguish progressive hair loss from diffuse or temporary thinning.
Genetics influence susceptibility, not certainty
Progressive hair loss occurs only in follicles that are genetically sensitive to androgens, particularly DHT. However, genetic predisposition does not determine:
- When progression begins
- How fast it advances
- Whether it becomes extensive
This variability explains why individuals with similar family histories can experience very different outcomes.
Time and comparison are essential
A single snapshot is rarely sufficient to diagnose progression. What matters is change over time.
- Stable thinning looks the same across repeated observations
- Progressive thinning shows consistent, directional change
- Baldness is the end result of untreated progression, not of thinning alone
For this reason, clinical evaluation often relies on baseline documentation and follow-up comparison, rather than isolated visual impressions. While doctors might bring you into
What this means at early stages
At early stages, progressive hair loss may still be limited and manageable. The goal of evaluation is to identify progression before irreversible loss occurs.
This does not mean treatment is always required. In some cases, monitoring is appropriate. In others, early intervention may help preserve existing hair.
The key point is that progressive thinning and non-progressive thinning require different decisions, even if they look similar initially.
When Hair Thinning Reflects Progressive Hair Loss
Perceived hair thinning becomes clinically significant when it reflects an active, progressive hair loss process, rather than a temporary or stable change in appearance.
What progresses is not thinning itself, but the biological condition causing that appearance — most commonly androgenetic alopecia.
What defines progressive hair loss clinically
Progressive hair loss is defined by ongoing follicle miniaturization.
In this process, hair follicles remain alive but gradually produce hairs that are:
- Shorter
- Finer
- Less pigmented
- Less capable of providing coverage
Over time, this results in visible density loss and, if untreated, baldness in affected areas.
Clinical features that suggest progression
When clinicians assess for progression, they look for:
- Patterned involvement
- Temples, frontal hairline, mid-scalp, or crown
- Localized density reduction
- Rather than diffuse thinning
- Variation in hair shaft diameter
- Finer hairs mixed with thicker terminal hairs
- Consistency across structured images
- Changes that align with known progression patterns
These features can often be identified through structured visual assessment interpreted clinically, even when changes are still subtle.
Why early progression is often underestimated
Early progressive hair loss rarely looks dramatic.
At initial stages:
- Many follicles remain functional
- Coverage is partially preserved
- Changes are incremental rather than obvious
Because of this, early androgenetic alopecia is frequently mistaken for benign thinning — especially without structured evaluation.
Genetics influence susceptibility, not inevitability
Genetic predisposition determines whether follicles are sensitive to androgens such as DHT.
It does not determine:
- How early progression begins
- How quickly it advances
- Whether it becomes extensive
This variability explains why individuals with similar family histories may experience very different outcomes.
The role of assessment at early stages
At early stages, assessment focuses on classification, not prediction.
When visual information is reviewed systematically — examining pattern, distribution, and hair shaft characteristics — clinicians can often determine whether miniaturization is present and assign an early stage.
In some cases, follow-up comparison adds confirmation. In others, a single structured evaluation is sufficient to guide monitoring or treatment decisions.
What this means for decision-making
When progressive hair loss is identified early:
- Options are broader
- Interventions can be conservative
- Monitoring may still be appropriate
When progression is not present, treatment is unnecessary.
The purpose of this distinction is not urgency, but appropriateness — ensuring that any next step aligns with the actual biological process.
Why Hair Thinning Is Often Misjudged Without Structure or Context
Perceived hair thinning is difficult to judge accurately through casual observation alone.
This is not because hair changes are unknowable, but because unstructured visual judgment is unreliable, particularly when changes are gradual.
For this reason, people often overestimate or underestimate change based on day-to-day appearance.
Factors that commonly distort perception
Several non-biological factors influence how dense hair appears at any given moment:
- Lighting conditions
- Direct or overhead light increases scalp visibility
- Hair length and styling
- Shorter or flatter styles reduce apparent volume
- Hair color and skin contrast
- Higher contrast increases perceived thinning
- Hair wetness or product use
- Wet or clumped hair exposes scalp
These variables change frequently and can create the impression of progression where none exists.
Why memory is an unreliable comparison point
Most people compare their hair to memory rather than documentation.
Because hair changes slowly, the brain tends to smooth over incremental differences. This makes it difficult to answer questions such as:
- “Has this area actually changed?”
- “Is this worse than last year?”
Without reference points, perception fills the gap.
Early progression may still be clinically identifiable
While casual observation is unreliable, structured visual assessment interpreted clinically is often sufficient to identify early progression .
At early stages:
- Density loss is localized rather than diffuse
- Miniaturized hairs coexist with thicker terminal hairs
- Pattern and distribution follow recognizable pathways
These features may not feel obvious subjectively, but they can be detected when images are reviewed systematically.
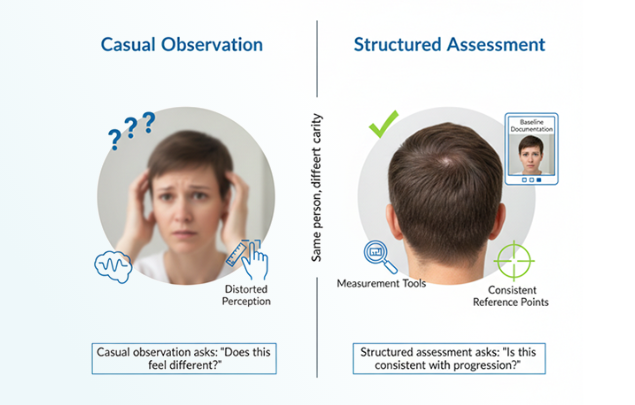
Why structure changes the answer
The difference between uncertainty and clarity is not time alone — it is context.
- Casual observation answers: “Does this feel different?”
- Structured assessment answers: “Is this consistent with progression?”
When findings are clear, additional waiting adds little. When findings are borderline, documentation over time provides confirmation.
What this means for early-stage decisions
Uncertainty does not mean progression.
But clarity often requires structured evaluation rather than repeated self-checking.
In many cases, assessment confirms stability. In others, it identifies early change at a stage when options remain flexible.
The goal is not vigilance — it is accuracy.
Treatment Options Based on the Underlying Cause
Treatment decisions are not based on the appearance of hair thinning.
They are based on what biological process has been identified , whether that process is active, and what can realistically be achieved at the current stage.
For this reason, treatment should be recommended by a doctor after medical review.
When treatment is not indicated
Treatment is often unnecessary when evaluation shows:
- The appearance of thinning reflects a non-progressive process
- Hair follicles are structurally intact
- Changes are stable or improving
- A temporary trigger has been identified and resolved
In these cases, intervention does not improve outcomes. Reassurance, observation, and time are appropriate medical responses.
When treatment may be considered
Treatment is considered when diagnosis identifies:
- Ongoing follicle miniaturization
- A pattern consistent with androgenetic alopecia
- Evidence of progressive change on structured assessment
At early stages, treatment aims to slow or stabilize progression, not to reverse hair loss or restore previous density.
What treatment can and cannot achieve
Treatment modifies progression. It does not change genetic susceptibility.
Depending on the individual and stage:
- Progression may slow or stop
- Existing hairs may become more stable or slightly thicker
- Cosmetic improvement may occur gradually
Significant change is unlikely to be immediate. Hair growth follows biological cycles, and visible effects typically require several months, not weeks.
Why timing influences options
Earlier identification allows for:
- Lower-intensity intervention
- Greater preservation of existing hair
- More conservative decision-making
Later stages limit what treatment can achieve, because follicles that have fully miniaturized cannot be reliably reactivated.
This is why treatment discussions are meaningful only after diagnosis, and why urgency is rarely appropriate.
Individual customized treatments matter
There is no universal treatment pathway.
Decisions depend on:
- The diagnosed process
- The extent and rate of progression
- Tolerance for monitoring versus intervention
- Personal priorities and expectations
Choosing not to treat is a valid decision when progression is absent or minimal.
How this fits into a diagnosis-led approach
Treatment is one possible outcome of evaluation — not the default.
In many cases, diagnosis leads to:
- Reassurance
- Monitoring
- Clear guidance on what does not require action
When treatment is appropriate, it is selected because it aligns with the biology and stage, not because thinning has been perceived.
When Hair Thinning Should Be Evaluated
Not every perceived change in hair density requires medical evaluation.
However, there are situations where seeking clarity is reasonable, particularly when the cause of thinning is unclear or when changes appear patterned or persistent.
The purpose of evaluation is not to confirm worst-case outcomes, but to determine whether the appearance of thinning reflects a stable process or an active one.
Situations where evaluation is often appropriate
Consider evaluation if one or more of the following apply:
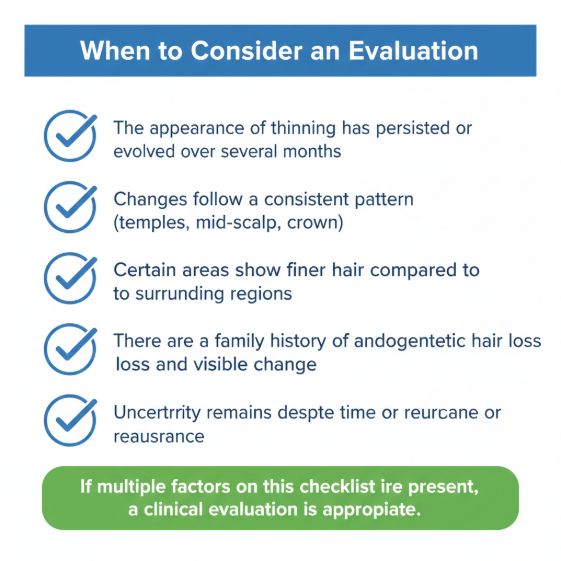
These factors do not indicate baldness. They indicate that assumptions have limits.
Situations where evaluation is usually not urgent
Immediate evaluation is often unnecessary when:
- Thinning appears diffuse and recent
- A clear temporary trigger is present
- Hair appearance is stable or improving
- Shedding has reduced or normalized
In these cases, observation is often sufficient.
What evaluation provides
Evaluation replaces uncertainty with structured information.
Specifically, it can:
- Identify whether the process is progressive or non-progressive
- Clarify pattern and stage
- Establish a baseline for future comparison
- Indicate whether monitoring or treatment is appropriate
In many cases, the outcome is reassurance rather than intervention.
Why waiting indefinitely is not the ideal option
While urgency is rarely appropriate, indefinite delay can narrow options.
Progressive hair loss advances gradually, and earlier stages offer more flexibility, including the option to monitor rather than act.
Evaluation allows decisions to be made with context instead of guesswork.
Advantages of getting a medical evaluation
If thinning remains unclear, a structured evaluation can help to:
- Confirm whether thinning is progressive or non-progressive
- Establish a baseline for future comparison
- Clarify which options — including doing nothing — are appropriate
Any next step should feel optional, informed, and medically appropriate.
Take a hair health assessment and get free consultation from a medical doctor in the EU to confirm your hair loss stage and next steps for hair regrowth.
How to Get Started
Hair thinning does not follow a single path.
For many individuals, the appearance of thinning stabilizes without intervention. For others, it reflects an early, gradual process that benefits from being identified sooner rather than later.
The purpose of understanding changes in your hair is not to predict worst-case outcomes, but to replace uncertainty with accurate context . When the underlying process is clear, decisions become simpler — whether that decision is to monitor, to reassess later, or to consider treatment.
No responsible approach begins with assumptions.
It begins with clarity.
Getting started simply involves confirming what process is causing the change you’re noticing and whether it is stable or progressive.
Take the Hair Assessment to have a doctor review your case, identify the underlying process, and assign an appropriate hair loss stage and next steps.

Add Comment