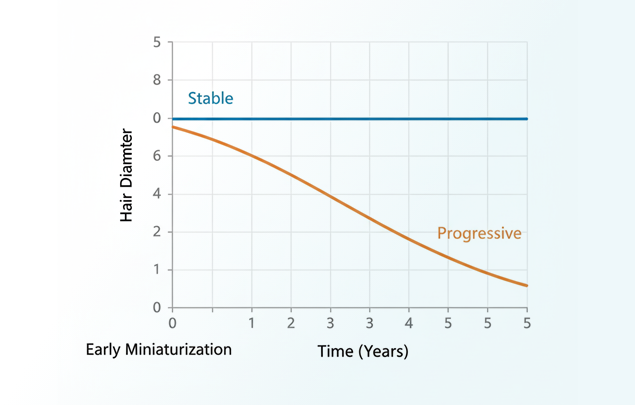
Hair thinning is one of the most common reasons people seek advice about hair changes — and one of the most misunderstood. For some individuals, reduced hair diameter remains stable for years without advancing. For others, it represents the earliest visible sign of progressive follicle miniaturization that will continue over time.
The challenge is that miniaturization does not follow a single timeline. The rate of change depends on underlying mechanism, follicle sensitivity to androgens, and whether the process is active or arrested. Shedding, miniaturization, and visible density loss are frequently confused, leading either to unnecessary concern or delayed evaluation.
This article explains how miniaturization progresses from a medical perspective, what influences its speed, and when evaluation is useful. The purpose is not to predict individual outcomes, but to replace uncertainty with accurate context — so decisions, whether to monitor or intervene, are based on mechanisms rather than assumption.
Shedding, Miniaturization, and Visible Density Loss
Early hair changes are difficult to interpret because different biological processes can look similar. These three terms describe distinct mechanisms with different implications.
| Term | Clinical Meaning | What It Reflects |
|---|---|---|
| Shedding | Hairs completing cycle and exiting scalp | Normal turnover, androgenetic alopecia (shortened cycles), telogen effluvium, anagen effluvium, or other cycling disorders |
| Miniaturization | Progressive reduction in hair shaft diameter and length | DHT-driven follicle changes in androgenetic alopecia |
| Visible density reduction | Reduced scalp coverage apparent on examination | Advanced miniaturization, reduced follicle count, or scarring processes |
Critical distinction: Shedding can occur with completely healthy follicles (telogen effluvium) or as a consequence of miniaturization (androgenetic alopecia). In androgenetic alopecia, affected follicles produce weaker hair with shorter growth cycles - this hair falls out sooner, creating increased daily shedding.
Miniaturization reflects changing follicle output; visible density reduction indicates sufficient miniaturization to affect cosmetic appearance.

What "Progression" Means Clinically
In androgenetic alopecia, "progression" refers specifically to continued miniaturization — ongoing reduction in hair shaft diameter and length over successive growth cycles. It does not describe sudden shedding or rapid disappearance of hair.
With each cycle, affected follicles produce hair that is finer, shorter, and less pigmented. Follicles remain biologically active and continue cycling, but their output declines gradually. This process occurs slowly and unevenly across the scalp, making early change difficult to detect without serial comparison.
| Follicle State | Biological Activity | Typical Observation |
|---|---|---|
| Normal activity | Full growth cycles, terminal hair production | Stable diameter and density |
| Active miniaturization | Shortened anagen, reduced diameter | Subtle caliber reduction, often without visible gaps |
| Advanced miniaturization | Repeated short cycles, vellus-like hairs | Noticeable density change, pattern emergence |
| Fibrotic/inactive | Minimal or absent production | Visible scalp, hair loss apparent |
Important: Miniaturization is not uniform. Some follicles remain stable while others progress, creating patterned rather than diffuse change. "Progression" specifically refers to continued diameter reduction in affected follicles, not universal scalp involvement.
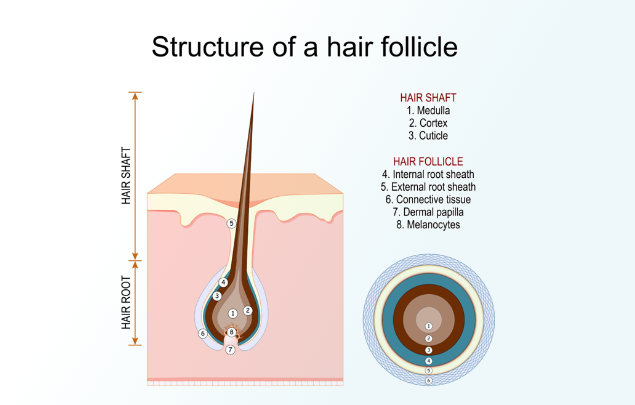
Diagram — Miniaturization Sequence
Single hair follicle shown across successive growth cycles, with each cycle producing a thinner, shorter hair shaft.
Progression vs. Shedding: Different Processes, Related in Androgenetic Alopecia
Progression (continued miniaturization) and increased shedding are frequently conflated because both involve visible hair fall. They reflect different biology—though in androgenetic alopecia, they are directly connected.
Shedding in healthy follicles = Hair completing normal cycle and exiting. Occurs with intact follicle function. Volume varies with cycle synchronization (telogen effluvium), stress, illness, or nutritional status. Does not indicate declining follicle capacity.
Shedding in androgenetic alopecia = Hair falling out because miniaturization has shortened the growth phase. The follicle cycles normally but produces hair with reduced lifespan. This is not damage or disease—it is the mechanical consequence of progressive diameter reduction. Androgenetic alopecia is the most common cause of pathological shedding.
Progression = Continued reduction in hair shaft diameter and length. Follicles cycle normally but produce progressively weaker hair with shorter anagen phases.
Why this matters: In telogen effluvium, shedding resolves when triggers pass and follicles return to full function. In androgenetic alopecia, shedding continues because the underlying miniaturization continues—each new cycle produces hair that falls out sooner than the last. This explains why hair count alone is unreliable for diagnosis. Evaluation focuses on diameter variation, caliber distribution, and whether shedding correlates with miniaturization patterns.
Biological Drivers of Progression
Progression in androgenetic alopecia reflects how follicles respond to DHT over time. DHT is a testosterone derivative present in all individuals; progression occurs only in genetically susceptible follicles.
Mechanism of miniaturization:
- Anagen (growth phase) progressively shortens
- Each cycle produces reduced diameter and length
- Follicle remains present and cycling
- Visible output declines gradually
Why patterns differ:
DHT sensitivity varies across the scalp based on genetic programming. This selective response creates recognizable patterns rather than uniform thinning. Areas with normal sensitivity maintain stable terminal hair; susceptible areas miniaturize.
Rate variability:
Progression speed differs between individuals due to:
- Degree of follicle sensitivity to DHT
- Local androgen concentration
- Age-related hormonal changes
- Scalp inflammatory environment
These factors influence when changes become noticeable, not whether miniaturization will occur.
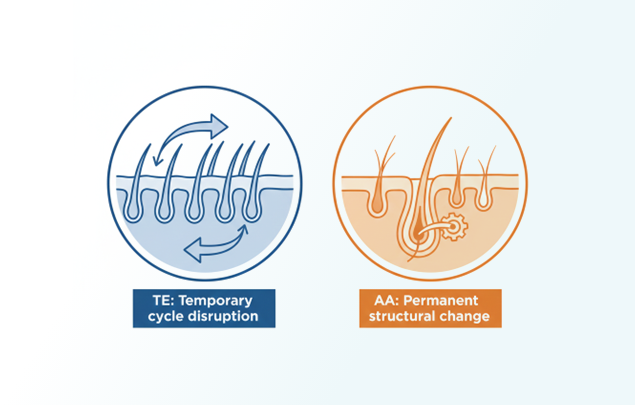
Shedding as a consequence: As anagen shortens, hair spends less time growing before entering the shedding phase. This creates the increased daily hair fall many patients notice first. Unlike telogen effluvium—where shedding signals temporary cycle disruption—in androgenetic alopecia, shedding signals structural follicle change. The same biological process (DHT-driven miniaturization) produces both reduced diameter and increased shedding.
Diagram — Mechanism (Simplified)
Testosterone converting to DHT, interacting with genetically sensitive follicles, leading to shortened growth cycles and reduced hair shaft thickness.
Understanding these biological drivers provides context for why hair loss progression is gradual, variable, and difficult to estimate without direct evaluation of follicle behavior.
Pattern Differences in Men and Women
Androgenetic alopecia produces different visible patterns in men and women, though the underlying miniaturization mechanism is identical.
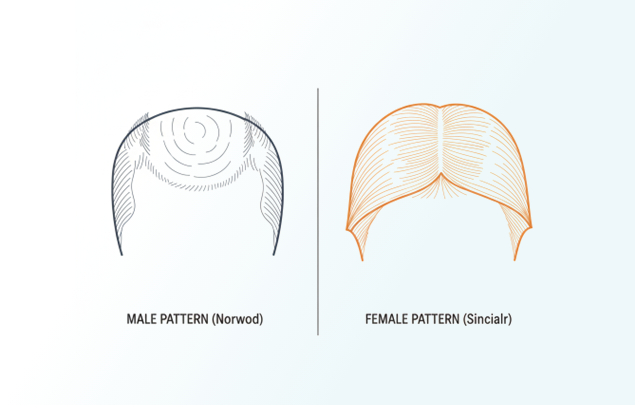
Male Pattern (Norwood Classification)
- Begins with temporal recession or vertex thinning
- Creates clear boundaries between affected and unaffected areas
- Frontal hairline often recedes
- Progression follows recognizable stages (Norwood 2–7)
Female Pattern (Sinclair Classification)
- Begins with central scalp thinning, part widening
- Diffuse density reduction without sharp boundaries
- Frontal hairline typically preserved
- Progression staged by central density (Sinclair 1–5)
Shared Characteristics
Both patterns involve:
- Miniaturization preceding visible density loss
- Phasic rather than continuous progression
- Poor correlation between shedding and advancement
- Need for serial comparison to assess change
Clinical note: Pattern classification (Norwood/Sinclair) describes distribution and extent of visible change. It does not indicate whether miniaturization is currently active or stable.
Diagram — Progression Timeline
Non-linear timeline showing long stable periods, subtle change, plateaus, and possible acceleration rather than continuous decline.
Understanding these patterns helps explain why early hair loss progression is often recognized retrospectively and why structured evaluation is more informative than casual observation.
When Miniaturization Is Stable
Miniaturization does not inevitably advance. Many individuals reach stable miniaturization — reduced but consistent hair diameter that remains unchanged for years.
Characteristics of stability:
- Hair caliber unchanged on serial assessment
- Density consistent within scalp regions over time
- No expansion of miniaturized zones
- Normal cycling with stable output
Clinical significance:
Stability indicates preserved follicle activity without continued deterioration. It allows monitoring without intervention and establishes realistic expectations. Stability is a valid outcome, not a missed opportunity.
When Miniaturization Is Progressive
Progressive miniaturization is defined by continued reduction in hair shaft diameter and length over time. This requires serial comparison for detection — isolated examination cannot establish progression.
Indicators of active progression:
- Reduced diameter on repeat calibrated assessment
- Expansion of miniaturized zones
- Increasing caliber variation within regions
- More defined pattern boundaries over time
Shedding does not indicate progression:
Shedding volume varies independently. Increased shedding may occur without miniaturization advancement; progression may continue with normal shed counts.
Note: While increased shedding often accompanies androgenetic alopecia, the volume of shed hair does not reliably indicate whether miniaturization is advancing. Shedding in AA reflects shortened growth cycles, not cycle disruption. Serial assessment of hair caliber—not shed counts—determines whether progression is occurring.
Why detection matters:
Identifying active progression while follicles remain capable of producing visible hair allows informed decision-making. Once miniaturization advances sufficiently to produce vellus hairs, reversal potential declines.
When Evaluation Provides Value
Not all hair changes require intervention. In many cases, the most useful step is confirming whether miniaturization is stable or active.
Evaluation is helpful when:
- Changes appear to be occurring but pattern is unclear
- Density differs from historical baseline under similar conditions
- Uncertainty exists about whether observed changes represent cycling variation or progressive miniaturization
- Monitoring alone no longer provides reassurance
What evaluation clarifies:
| Finding | Implication |
|---|---|
| Stable miniaturization | Continued monitoring appropriate; no active progression |
| Active progressive miniaturization | Informed discussion of options while follicle capacity preserved |
| Advanced miniaturization | Realistic expectations about intervention potential |
Each outcome is clinically meaningful. None requires urgent action.
What evaluation does not do:
Evaluation does not commit to treatment, predict future progression, or guarantee outcomes. It provides mechanism-based context for decision-making.
Next Step
Hair changes are best understood through assessment of follicle status rather than assumption. If you are observing changes in hair caliber, density, or coverage, structured evaluation can clarify whether miniaturization is stable or progressive and what this means for your specific situation.
Take the Hair Assessment to have a physician evaluate your pattern, determine whether miniaturization is active or stable, and provide appropriate clinical context for next steps.

Add Comment