
Hair disorders are often discussed casually online, but medically they represent a large and complicated group of conditions with very different causes, behaviours, and treatments.
Two people may both describe “hair loss” while actually having entirely different diseases. One may have temporary stress-related shedding. Another may have an autoimmune condition. A third may have permanent scarring destruction of the follicles.
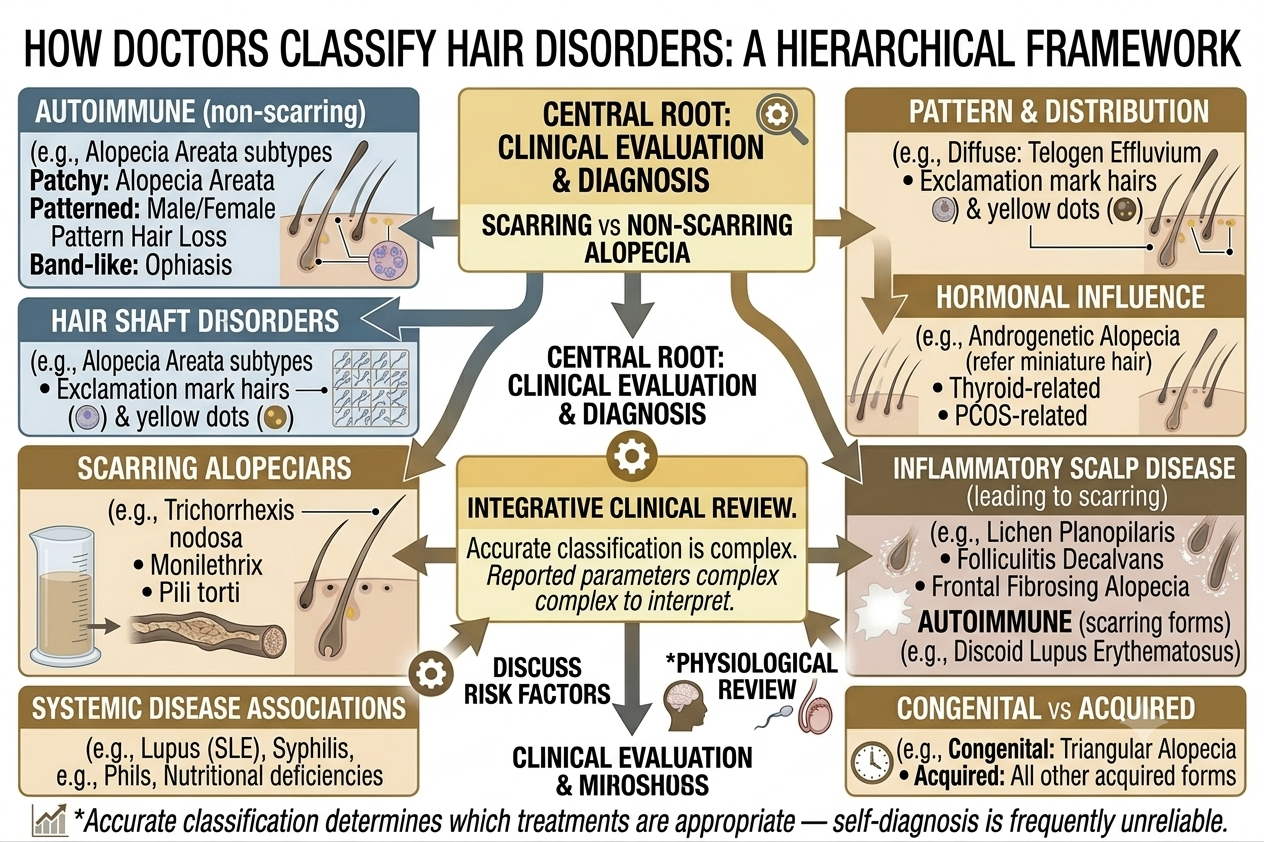
This is why dermatologists classify hair disorders systematically rather than treating all thinning as the same problem.
Classification helps doctors determine:
- Whether follicles are still alive
- Whether hair loss may reverse
- Whether inflammation is present
- Whether systemic disease may be involved
- Which treatments are appropriate
Understanding these categories also helps explain why some treatments work well for one disorder yet fail completely in another.
Hair disorders are not all forms of alopecia
The word alopecia simply means hair loss.
But hair disorders include far more than visible shedding alone. Some conditions primarily affect:
Hair growth rate
Hair texture
Hair shaft structure
Scalp inflammation
Excess hair growth
Fragility
Classification therefore extends beyond baldness itself.
One major division is scarring versus non-scarring hair loss
This distinction is one of the most important in dermatology.
In non-scarring alopecia, follicles remain structurally capable of producing hair even if cycling becomes abnormal.
In scarring alopecia, inflammation destroys follicles and replaces them with scar tissue. Once this occurs, regrowth becomes far more difficult or impossible.
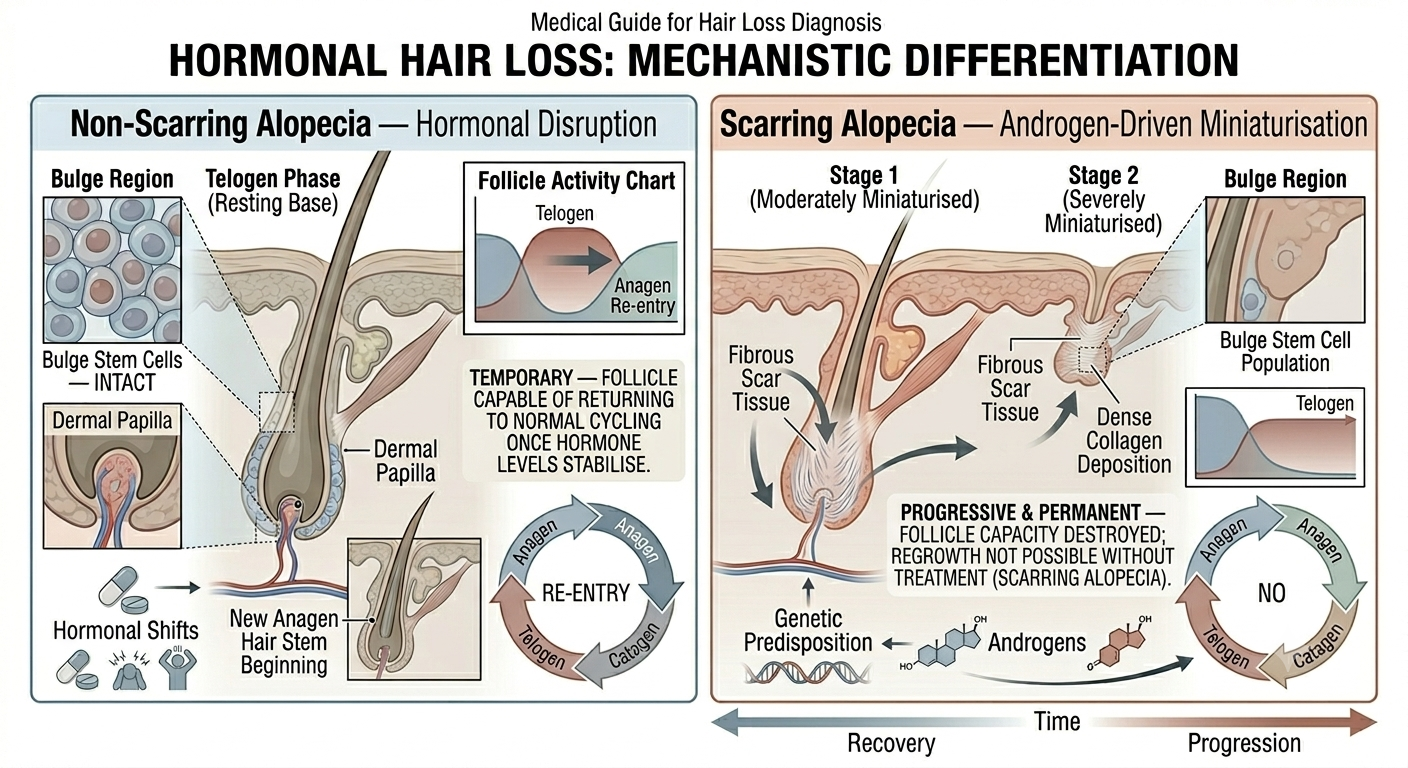
Early recognition matters because untreated scarring disease may lead to permanent loss.
Non-scarring alopecia is more common
Most common hair loss conditions are non-scarring.
Examples include:
Androgenetic alopecia
Telogen effluvium
Alopecia areata
Traction alopecia in early stages
In these disorders, follicles are usually still present beneath the skin.
This is one reason treatment and recovery are often at least partially possible.
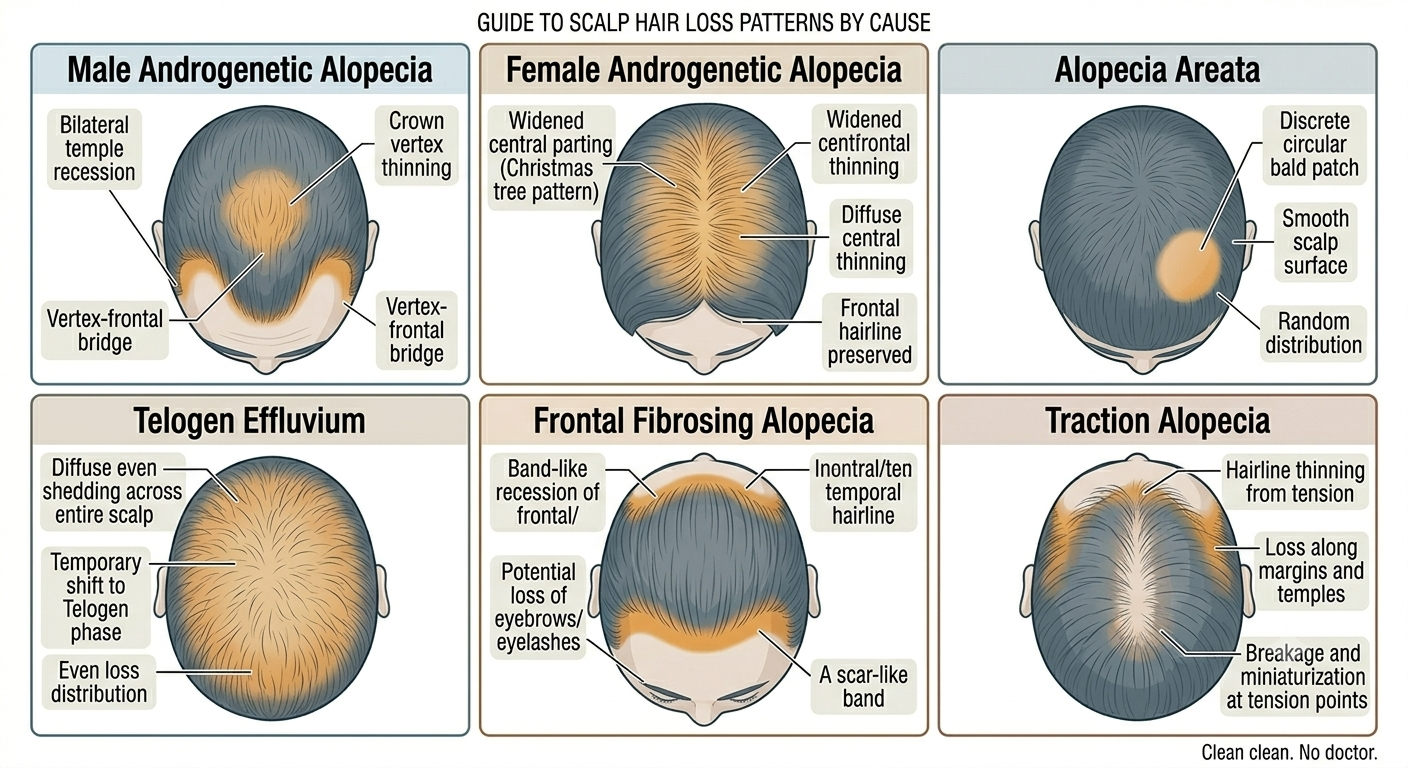
Androgenetic alopecia is pattern hair loss
Androgenetic alopecia is the most common form of progressive hair loss in adults.
In men, it often causes:
Receding temples
Vertex thinning
Progressive crown loss
In women, thinning more commonly appears as diffuse widening through the central scalp while preserving the frontal hairline initially.
The condition involves genetically sensitive follicles gradually miniaturising under androgen influence.
Doctors classify severity using systems such as:
The Norwood scale in men
The Ludwig scale in women
These scales help track progression over time.
Telogen effluvium is a shedding disorder
Telogen effluvium involves abnormal shifting of hairs into the resting phase of the growth cycle.
It commonly occurs after:
Illness
Stress
Childbirth
Rapid weight loss
Nutritional deficiency
Surgery
Rather than causing distinct bald patches, telogen effluvium usually produces diffuse shedding across the scalp.
Importantly, the follicles themselves are not permanently destroyed.
Alopecia areata is an autoimmune condition
Alopecia areata occurs when the immune system targets hair follicles.
It classically causes smooth round patches of sudden hair loss, though patterns vary considerably.
Subtypes include:
Patchy alopecia areata
Alopecia totalis involving the entire scalp
Alopecia universalis involving body hair
Follicles usually remain alive despite immune attack, meaning regrowth can occur even after extensive loss.
However, the disease course is unpredictable.
Scarring alopecias are medically more urgent
Scarring alopecias involve inflammatory destruction of follicles.
Examples include:
Lichen planopilaris
Frontal fibrosing alopecia
Central centrifugal cicatricial alopecia
Discoid lupus erythematosus
Symptoms may include:
Burning
Pain
Itching
Scalp redness
Loss of follicular openings
Because permanent damage may occur, these conditions often require early specialist management.
Doctors also classify disorders by distribution pattern
The pattern of loss provides important diagnostic clues.
Hair disorders may appear as:
Diffuse thinning
Patchy loss
Frontal recession
Crown thinning
Band-like patterns
Localised areas behind the ears or temples
Pattern recognition helps narrow the differential diagnosis considerably.
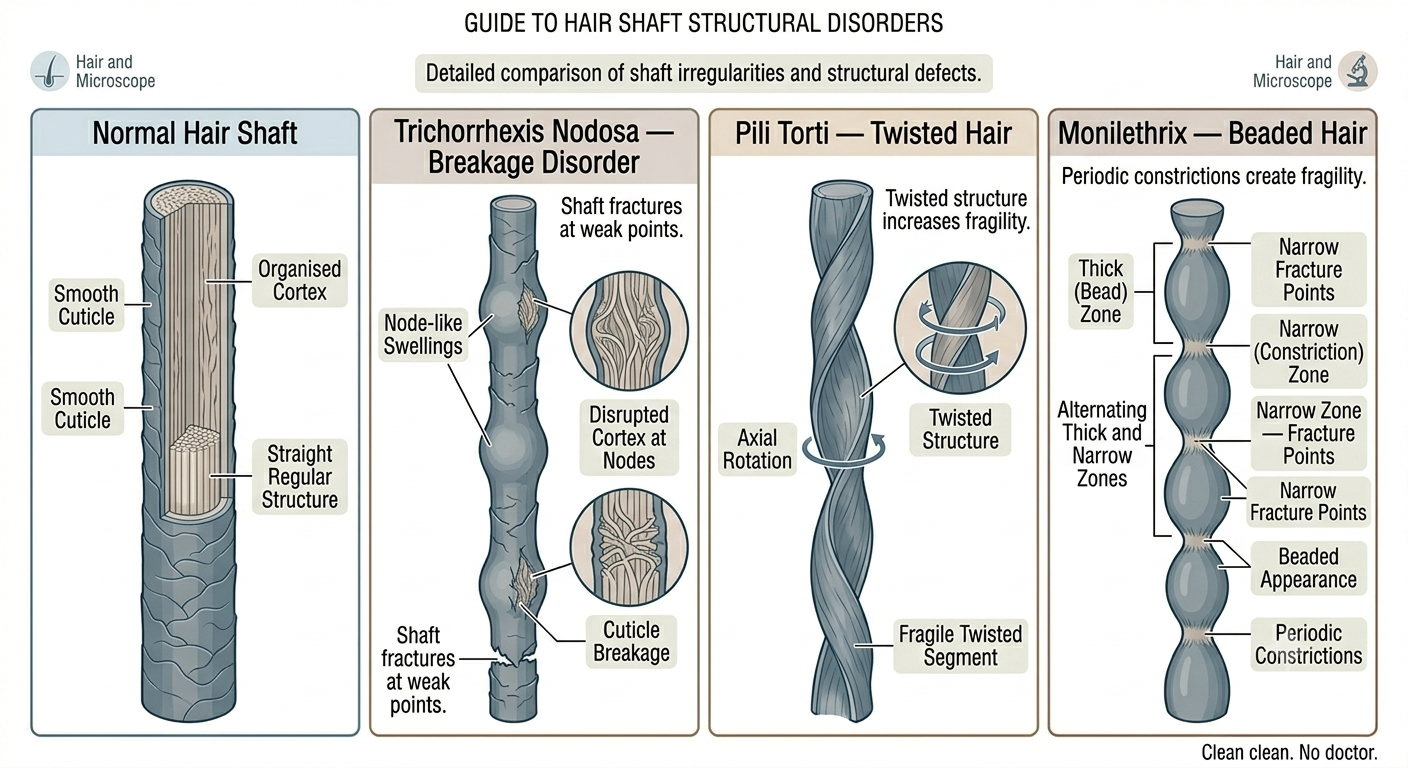
Hair shaft disorders are a separate category
Not all hair problems originate from the follicle.
Some disorders primarily affect the structure of the hair shaft itself, causing fragility or abnormal texture.
Examples include conditions causing:
Easy breakage
Twisted hairs
Beaded hairs
Brittle shafts
Some shaft disorders are inherited. Others result from chemical damage, nutritional deficiency, or systemic disease.
Congenital versus acquired disorders
Doctors also distinguish between conditions present from birth and those acquired later.
Congenital hair disorders often involve genetic abnormalities affecting:
Follicle development
Hair shaft formation
Keratin structure
Acquired disorders develop later because of hormonal, autoimmune, inflammatory, infectious, or environmental factors.
The timing of onset can therefore be diagnostically important.
Hormonal hair disorders form another category
Hormones strongly influence follicle behaviour.
Disorders involving hormonal imbalance may include:
Female pattern hair loss
Hair loss associated with polycystic ovary syndrome
Thinning related to thyroid disease
Some hormonal conditions cause scalp thinning while simultaneously increasing facial or body hair growth.
This combination can provide useful clinical clues.
Inflammatory scalp disease may affect hair indirectly
Some scalp conditions are not primarily hair diseases but still disrupt follicles through inflammation.
Examples include:
Seborrhoeic dermatitis
Psoriasis
Folliculitis
These conditions may increase shedding, irritation, or breakage even if they do not directly miniaturise follicles in the same way as androgenetic alopecia.
Traction alopecia sits between mechanical and follicular disease
Traction alopecia develops from chronic tension on the hair.
Tight hairstyles may gradually damage follicles over time.
Early stages are often reversible if tension stops. Longstanding traction, however, may eventually produce permanent follicular loss resembling scarring alopecia.
This progression illustrates why classification sometimes overlaps rather than fitting perfectly into rigid boxes.
Hair disorders may reflect systemic illness
Some hair abnormalities signal broader medical problems.
Doctors may investigate systemic causes when hair changes accompany:
Fatigue
Weight loss
Rashes
Joint symptoms
Anaemia
Hormonal changes
The scalp can sometimes act as an external marker of internal disease.
Classification guides treatment choices
Different disorders require completely different management approaches.
For example:
Finasteride may help androgenetic alopecia
Steroids may help alopecia areata
Anti-inflammatory treatment may help scarring disease
Nutritional correction may help deficiency-related shedding
Using the wrong treatment for the wrong disorder may waste time while disease progresses.
Biopsy is sometimes necessary
Clinical examination alone is not always enough.
When diagnosis remains uncertain, dermatologists may perform scalp biopsy to examine follicular architecture and inflammatory patterns microscopically.
Biopsy is especially useful in suspected scarring alopecia where treatment urgency matters.
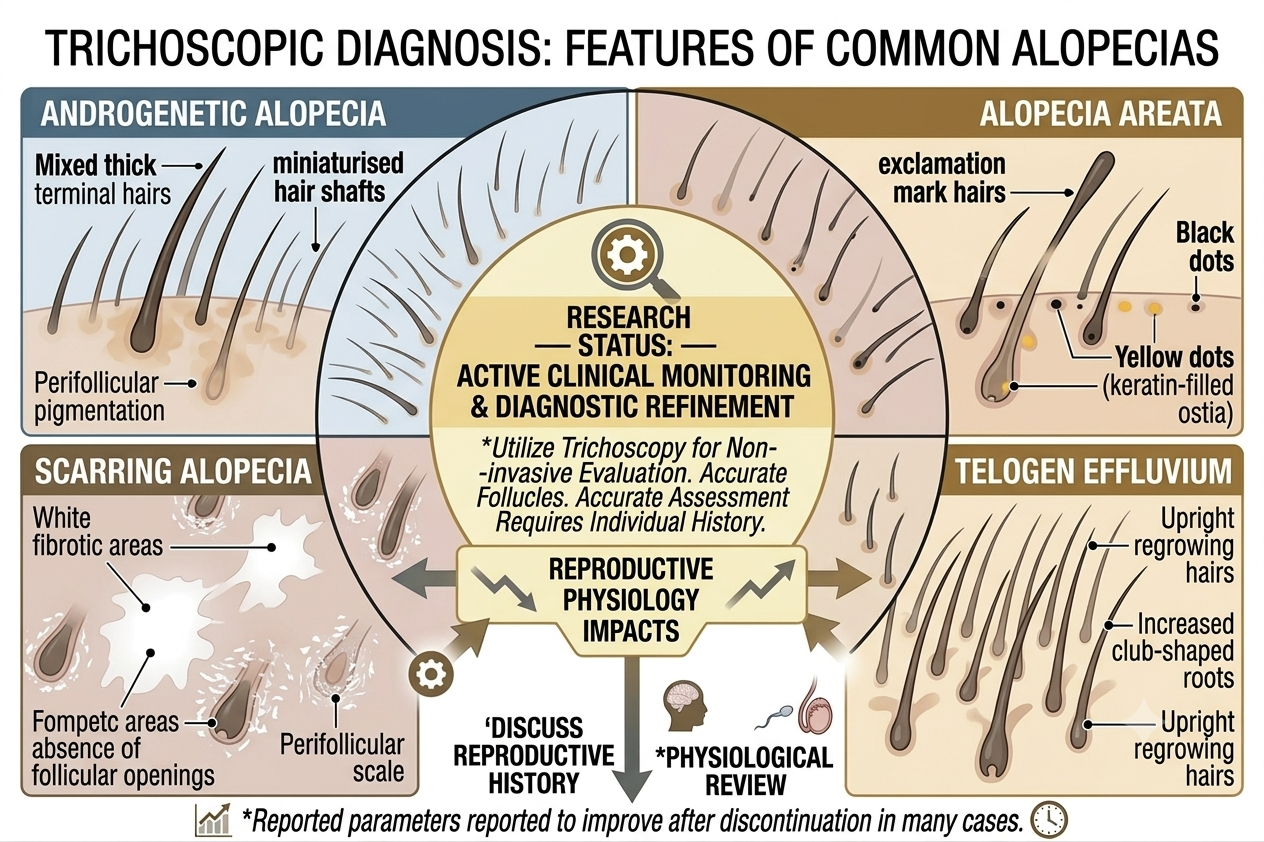
Trichoscopy has become increasingly important
Modern hair specialists frequently use trichoscopy, a form of scalp magnification.
This allows visualisation of:
Miniaturised hairs
Inflammatory changes
Follicular openings
Broken hairs
Scalp vascular patterns
Trichoscopy helps improve diagnostic accuracy without invasive procedures in many cases.
Hair disorders often overlap
Real patients do not always fit neatly into textbook categories.
Someone may simultaneously have:
Androgenetic alopecia
Telogen effluvium
Seborrhoeic dermatitis
This overlap partly explains why diagnosis and treatment can become complicated.
Online self-diagnosis is often unreliable
Because many hair disorders produce visually similar thinning, self-diagnosis based solely on internet photos is frequently inaccurate.
Patchy loss may reflect:
Alopecia areata
Traction
Fungal infection
Scarring disease
Diffuse shedding may stem from stress, iron deficiency, thyroid disease, medications, or pattern hair loss.
Proper assessment often requires broader clinical context.
The bottom line
Doctors classify hair disorders in several important ways, including scarring versus non-scarring disease, pattern and distribution of loss, inflammatory involvement, hormonal influence, and hair shaft abnormalities.
This classification system matters because different disorders behave differently and require very different treatments. Some forms of hair loss are temporary and reversible. Others may lead to permanent follicular destruction if not recognised early.
Hair loss is therefore not a single disease but a broad medical category containing many distinct conditions. Accurate diagnosis remains one of the most important parts of effective treatment.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.

Add Comment