
Hormonal contraception affects far more than fertility. Birth control pills influence hormone levels throughout the body, including the scalp and hair follicles. For some women, hormonal contraception improves hair stability. For others, it may contribute to shedding or worsening pattern hair loss.
This can make the subject deeply confusing.
One person may notice fuller hair after starting the pill, while another experiences significant thinning months later. Both experiences can be real because the relationship between hormones and hair is highly individual.
The type of pill matters. The hormonal sensitivity of the follicles matters. Genetics matter. Timing matters too.
Understanding how different contraceptives interact with hair biology helps explain why some pills are considered lower risk for hair loss than others.
Hair follicles respond to hormones
Hair follicles are hormonally sensitive structures.
Androgens, particularly dihydrotestosterone or DHT, play an important role in androgenetic alopecia, also called female pattern hair loss. In genetically susceptible individuals, androgens can gradually shrink follicles over time.
Some hormonal contraceptives reduce androgen activity. Others may have androgen-like effects themselves.
This difference is central to understanding why hair responses vary between pills.
Combined pills contain both oestrogen and progestin
Most oral contraceptive pills contain:
An oestrogen component
A synthetic progesterone-like hormone called a progestin
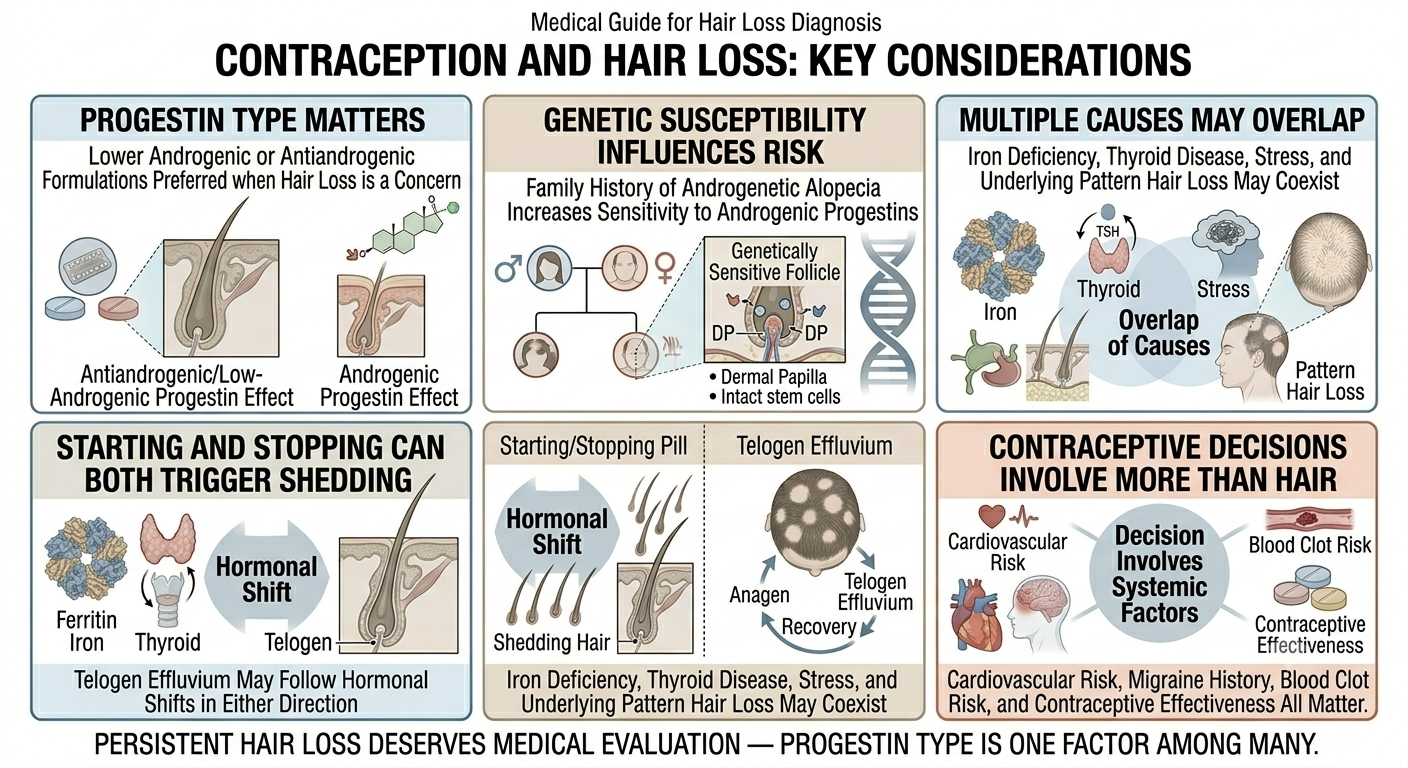
The progestin type matters significantly because different progestins have different androgenic properties.
Some behave more like androgens biologically. Others have lower androgenic activity or even antiandrogenic effects.
This is why two contraceptive pills can affect hair very differently despite both being classified as “the pill”.
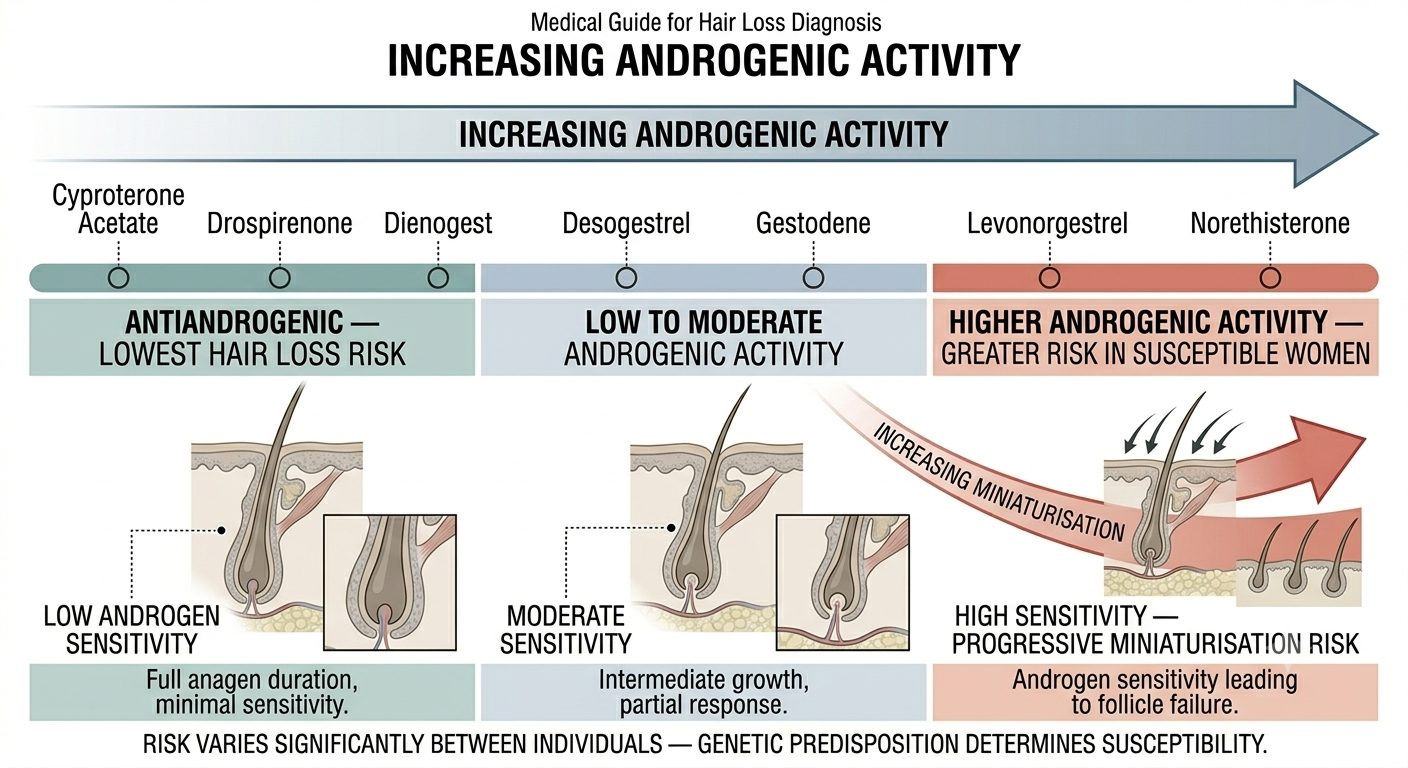
Higher androgenic progestins may increase risk
Certain progestins are considered more androgenic, meaning they may mimic some androgen effects more strongly.
Examples often considered relatively more androgenic include:
Levonorgestrel
Norethisterone
Desogestrel to a lesser degree in some contexts
These pills do not automatically cause hair loss in most users. But in genetically susceptible women, they may potentially worsen androgen-sensitive hair thinning.
Risk varies substantially between individuals.
Lower androgenic or antiandrogenic pills may be preferred in hair loss
Some contraceptives are considered more hair-friendly because of lower androgenic activity.
Examples may include formulations containing:
Drospirenone
Cyproterone acetate in certain regions
Dienogest
These are sometimes chosen for women with:
Acne
Hirsutism
Polycystic ovary syndrome
Androgen-sensitive hair thinning
However, no contraceptive should be viewed as a guaranteed hair treatment. Hormonal responses remain individual.
Oestrogen can prolong the growth phase
Oestrogen tends to support longer hair growth cycles.
This partly explains why many women notice fuller hair during pregnancy, when oestrogen levels are elevated. When hormone levels later shift downward, increased shedding often follows.
Combined oral contraceptives may stabilise hormones in ways that reduce shedding for some women.
But this effect is not universal.
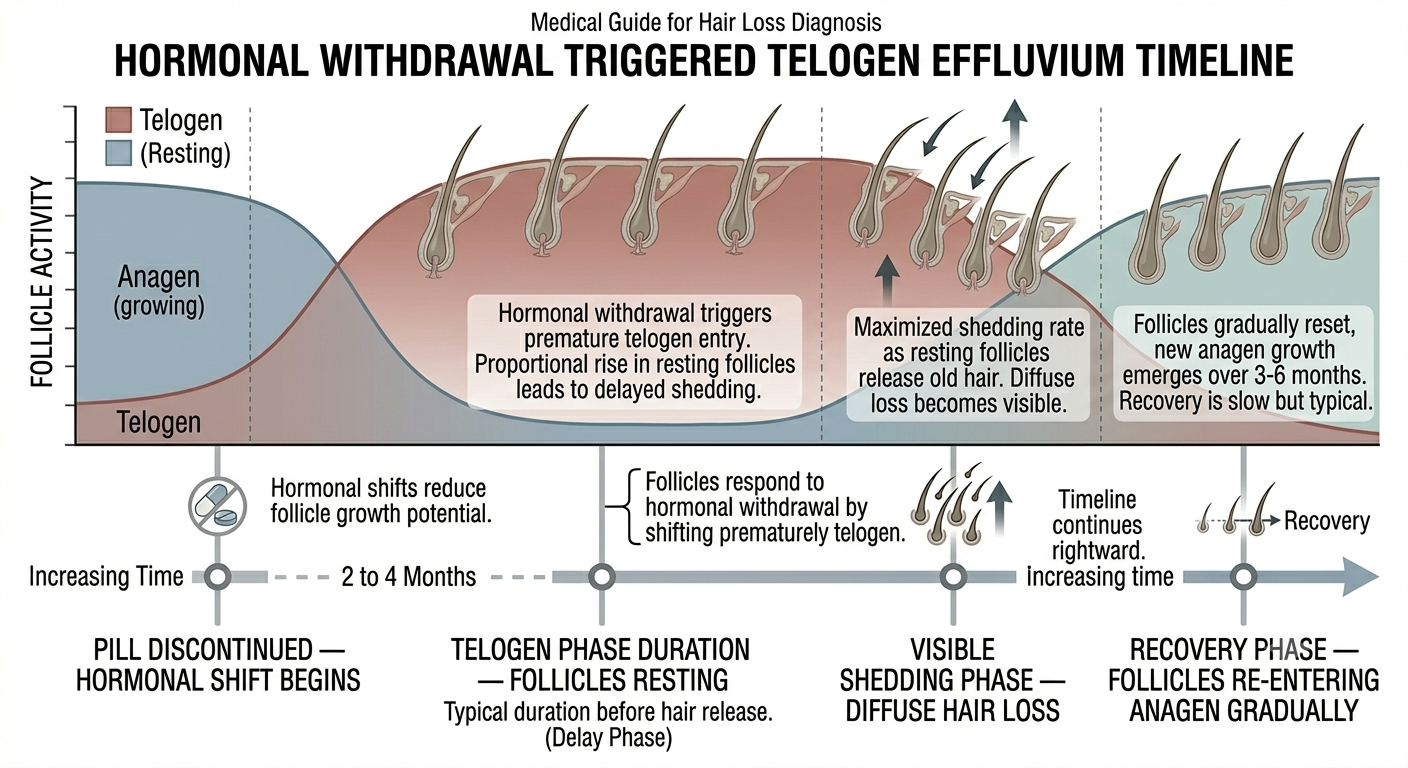
Stopping the pill can also trigger shedding
Hair shedding is not only associated with starting contraception.
Some women experience telogen effluvium after stopping hormonal birth control because follicles respond to the hormonal shift itself.
This type of shedding usually appears several months after discontinuation because hair cycles operate slowly.
The timing often causes confusion because the connection to the pill may not be immediately obvious.
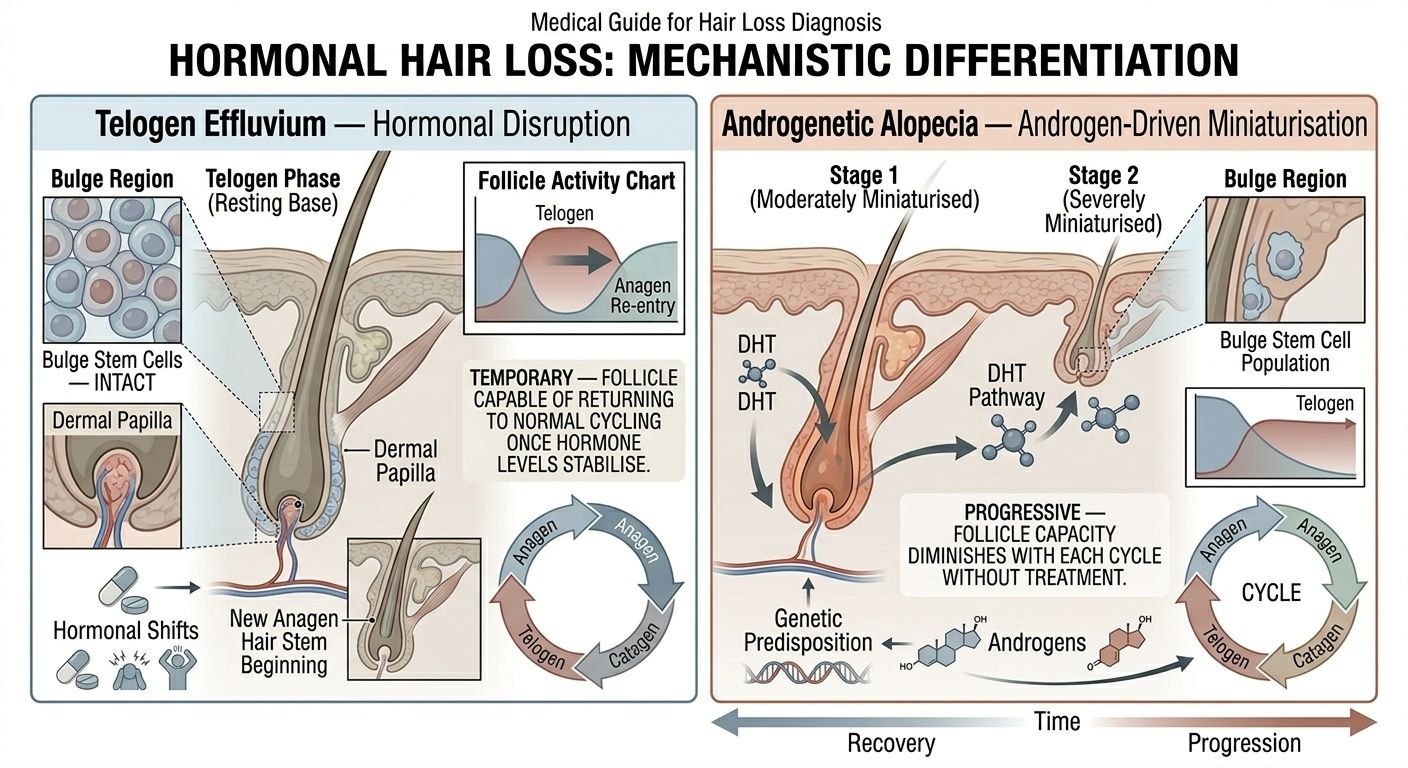
Telogen effluvium is different from androgenetic alopecia
Hormonal contraceptives may contribute to two very different hair problems.
The first is telogen effluvium, where many follicles shift into a resting phase after hormonal disruption. This causes diffuse shedding.
The second is androgen-sensitive miniaturisation in genetically predisposed women, which resembles female pattern hair loss.
The distinction matters because:
Telogen effluvium is often temporary
Androgenetic alopecia may progressively worsen over time
The treatments and prognosis differ.
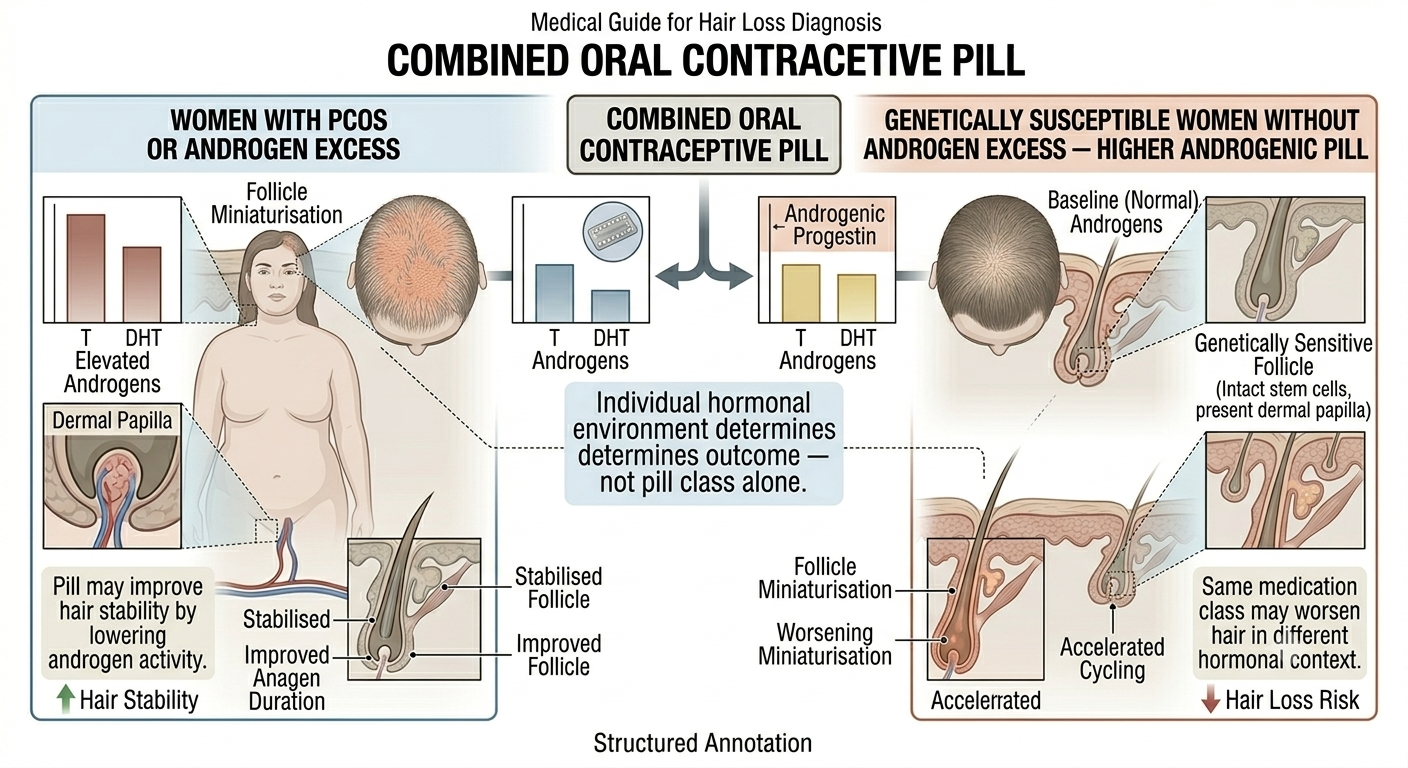
Polycystic ovary syndrome complicates the picture
Many women taking hormonal contraception already have underlying hormonal conditions such as polycystic ovary syndrome, or PCOS.
PCOS itself may contribute to:
Hair thinning
Acne
Excess facial hair
Irregular cycles
In these cases, a pill may actually improve hair stability by reducing androgen effects.
This creates a paradox where the same medication class may worsen hair in one woman while improving it in another.
Progesterone-only contraception may affect hair differently
Not all contraception contains oestrogen.
Progesterone-only pills, hormonal coils, injections, and implants may influence hair differently depending on the formulation and the individual’s hormonal sensitivity.
Some women report increased shedding with progesterone-only methods, particularly if they are already predisposed to androgenetic alopecia.
However, evidence remains variable and not all users experience problems.
Hair loss after starting contraception is not always caused by the pill
Timing alone does not prove causation.
Hair loss may coincide with:
Stress
Nutritional deficiency
Postpartum hormonal change
Thyroid disease
Weight loss
Underlying androgenetic alopecia
Because hair shedding often appears months after a trigger, identifying the true cause is not always straightforward.
This is one reason proper medical assessment matters in persistent or severe cases.
Family history matters
Women with a strong family history of androgenetic alopecia may be more hormonally sensitive regarding scalp hair.
In these individuals, highly androgenic contraceptives may theoretically pose greater risk than in women without genetic predisposition.
Again, this is not absolute. Many genetically susceptible women tolerate hormonal contraception without noticeable hair effects.
The pill is not a universal hair treatment
Some online discussions portray certain contraceptives as straightforward hair growth solutions.
The reality is more complicated.
Hormonal contraception may help stabilise hair in selected women, especially when androgen excess contributes to thinning. But the pill is not primarily a hair medication, and responses remain highly individual.
Some women improve. Others worsen. Some notice no difference at all.
Hair changes may take months to appear
Because hair follicles cycle slowly, hormonal hair changes are delayed.
This means:
Hair loss may begin months after starting a pill
Shedding may continue temporarily after stopping it
Improvement after changing pills may also take time
People often expect immediate effects that do not match follicle biology.
Switching pills should involve medical guidance
Women concerned about hair changes should not abruptly stop contraception without discussing alternatives with a healthcare professional.
Contraceptive decisions involve many factors beyond hair, including:
Cardiovascular risk
Migraine history
Smoking status
Blood clot risk
Endometriosis
Cycle control
Contraceptive effectiveness
Hair considerations matter, but they are only one part of the overall decision.
Severe shedding deserves broader evaluation
Significant hair loss should not automatically be blamed entirely on contraception.
Medical assessment may still be appropriate to evaluate:
Iron deficiency
Thyroid dysfunction
Autoimmune disease
Nutritional deficiency
Underlying androgenetic alopecia
Multiple factors commonly overlap.
Online fear around contraception and hair is often oversimplified
Discussions online frequently become polarised.
Some sources claim the pill destroys hair universally. Others dismiss all reports of contraceptive-related shedding entirely.
Neither position reflects the complexity of real clinical practice.
Hormonal contraception can influence hair biology, but effects vary widely depending on genetics, formulation, hormonal environment, and individual susceptibility.
The bottom line
Birth control pills can affect hair because hair follicles are hormonally sensitive. Pills containing more androgenic progestins may carry greater theoretical risk of worsening androgen-sensitive hair thinning in susceptible women, while lower androgenic or antiandrogenic formulations may sometimes be preferred in women with acne, PCOS, or pattern hair loss.
At the same time, hormonal shifts from starting or stopping contraception can trigger temporary telogen effluvium even without permanent follicle damage.
Hair responses to contraception are highly individual. Persistent or severe hair loss deserves proper medical evaluation rather than assumptions based solely on the timing of contraceptive use.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.

Add Comment