Hair loss is often treated as an isolated cosmetic problem. But when significant hair shedding appears alongside extreme fatigue, the picture changes. The combination can point toward broader systemic issues affecting the body well beyond the scalp.
This does not mean every tired person with hair loss has a serious illness. Fatigue is extremely common, and many forms of hair loss are unrelated to internal disease. But persistent exhaustion together with noticeable shedding deserves a more medically grounded assessment than simply changing shampoos or starting supplements at random.
Hair follicles are biologically active structures. They respond to hormonal shifts, nutritional status, inflammation, illness, stress, and metabolic disruption. When the body is under strain, hair growth is often affected early because follicles are not essential for survival.
That is one reason hair loss sometimes becomes a visible clue that something more systemic is happening.
Telogen effluvium is commonly linked to systemic stress
One of the most common forms of diffuse shedding associated with fatigue is telogen effluvium.
In telogen effluvium, a larger-than-normal number of follicles prematurely enter the resting phase of the hair cycle after a physiological or psychological stressor.
Potential triggers include:
Severe illness
Major surgery
Nutritional deficiency
Rapid weight loss
High fever
Hormonal disruption
Significant emotional stress
Because hair cycling is delayed, shedding often appears several months after the original trigger.
The fatigue may therefore begin before the hair loss becomes obvious.
Iron deficiency is a major possibility
Iron deficiency is one of the most important causes to investigate when fatigue and hair shedding occur together.
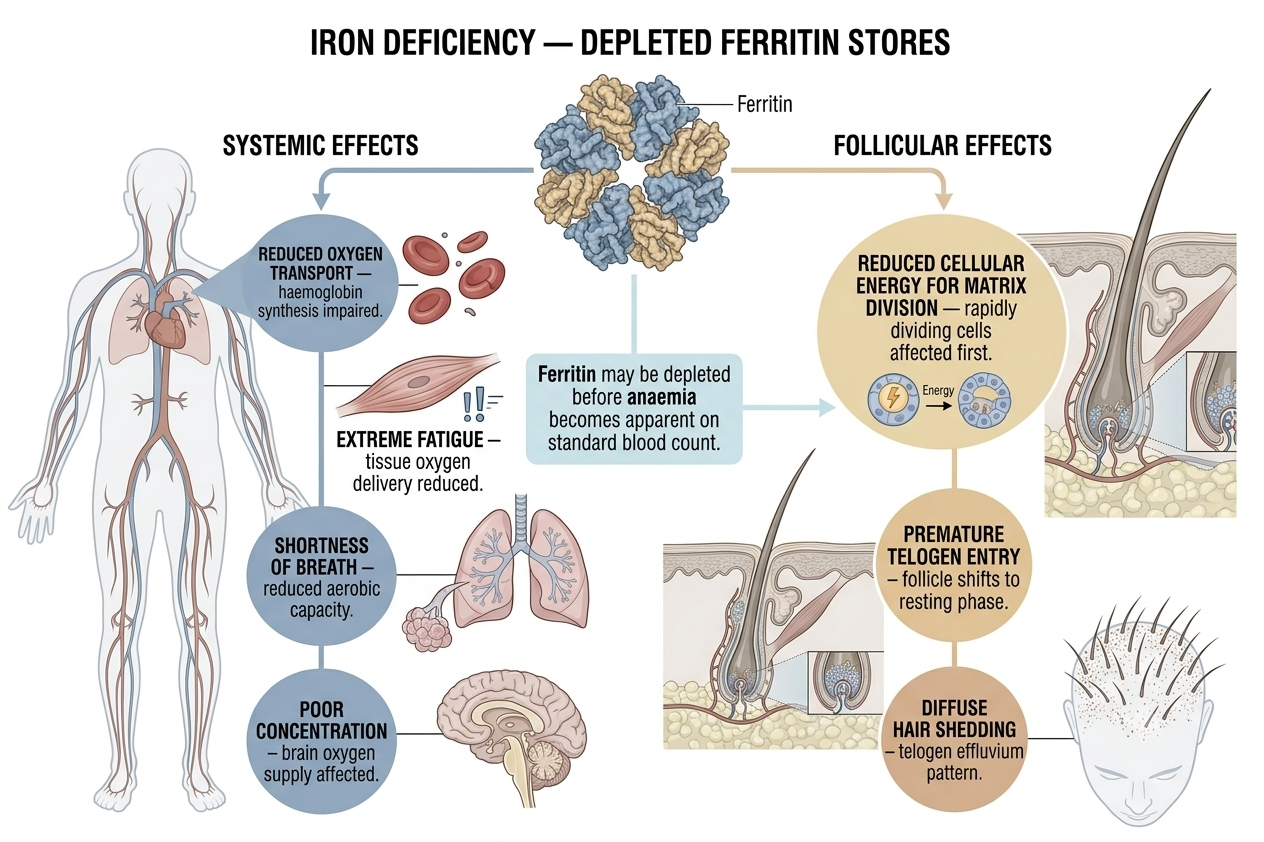
Iron plays a central role in oxygen transport and cellular metabolism. Low iron stores may contribute to:
Exhaustion
Shortness of breath
Poor concentration
Hair shedding
Reduced exercise tolerance
Brittle nails
Some individuals develop iron deficiency without obvious anaemia initially. Ferritin levels, which reflect iron storage, may become depleted before haemoglobin falls significantly.
Heavy menstrual bleeding, restricted diets, gastrointestinal conditions, and chronic blood loss are common contributors.
Anaemia itself may contribute to hair changes
Anaemia refers to reduced oxygen-carrying capacity in the blood.
When tissues receive less oxygen, rapidly dividing structures like hair follicles may be affected. Hair growth may slow, shedding may increase, and strands may appear finer or more fragile.
Anaemia has multiple possible causes beyond iron deficiency, including:
Vitamin B12 deficiency
Folate deficiency
Chronic inflammatory disease
Kidney disease
Bone marrow disorders
Proper medical evaluation matters because treatment depends on the underlying cause.
Thyroid disease frequently affects both energy and hair
The thyroid gland strongly influences metabolism and follicle function.
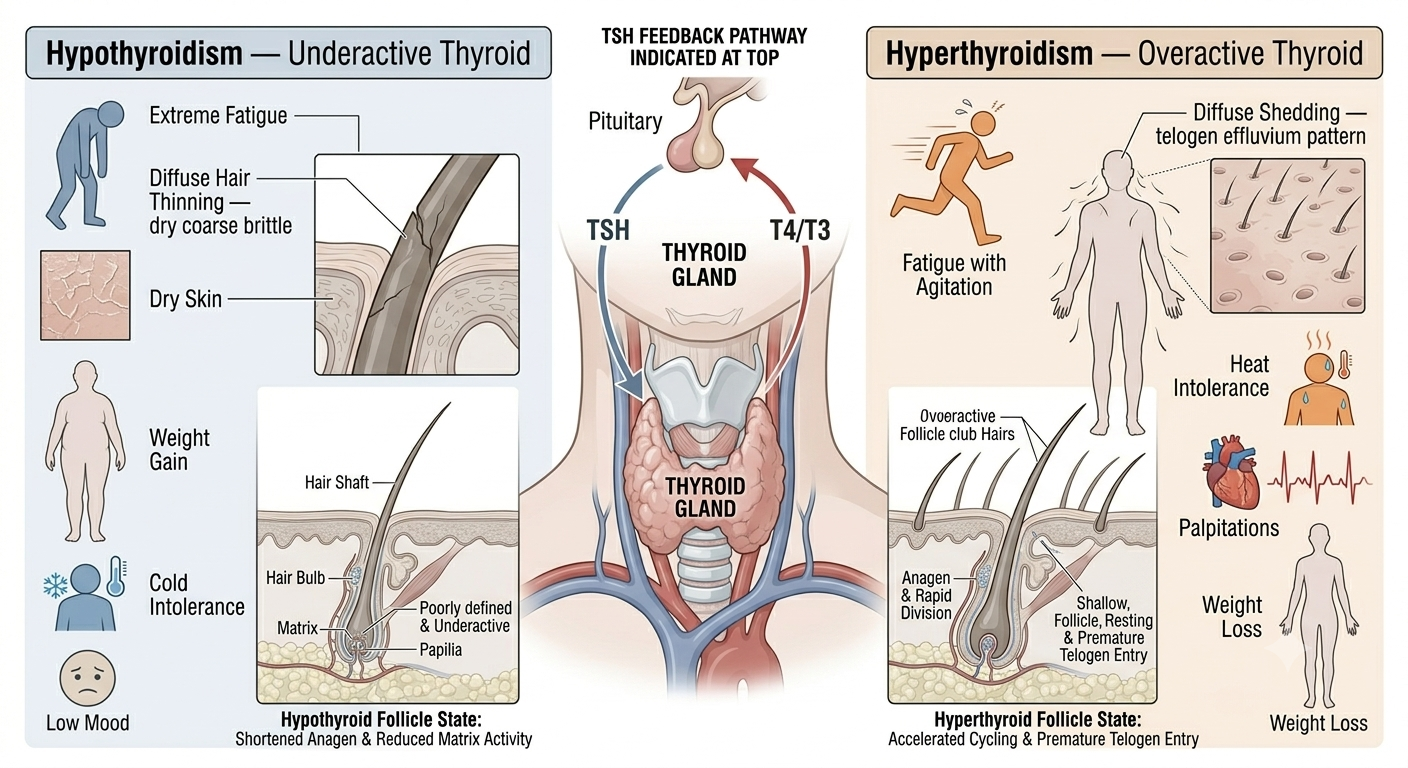
Hypothyroidism in particular may cause:
Extreme tiredness
Diffuse hair thinning
Dry skin
Weight gain
Cold intolerance
Constipation
Low mood
Hair associated with hypothyroidism often becomes dry, coarse, or brittle in addition to thinning.
Hyperthyroidism can also trigger shedding, although symptoms differ and may include heat intolerance, palpitations, and weight loss.
Because thyroid disorders are common and treatable, thyroid testing is frequently appropriate in unexplained fatigue with hair changes.
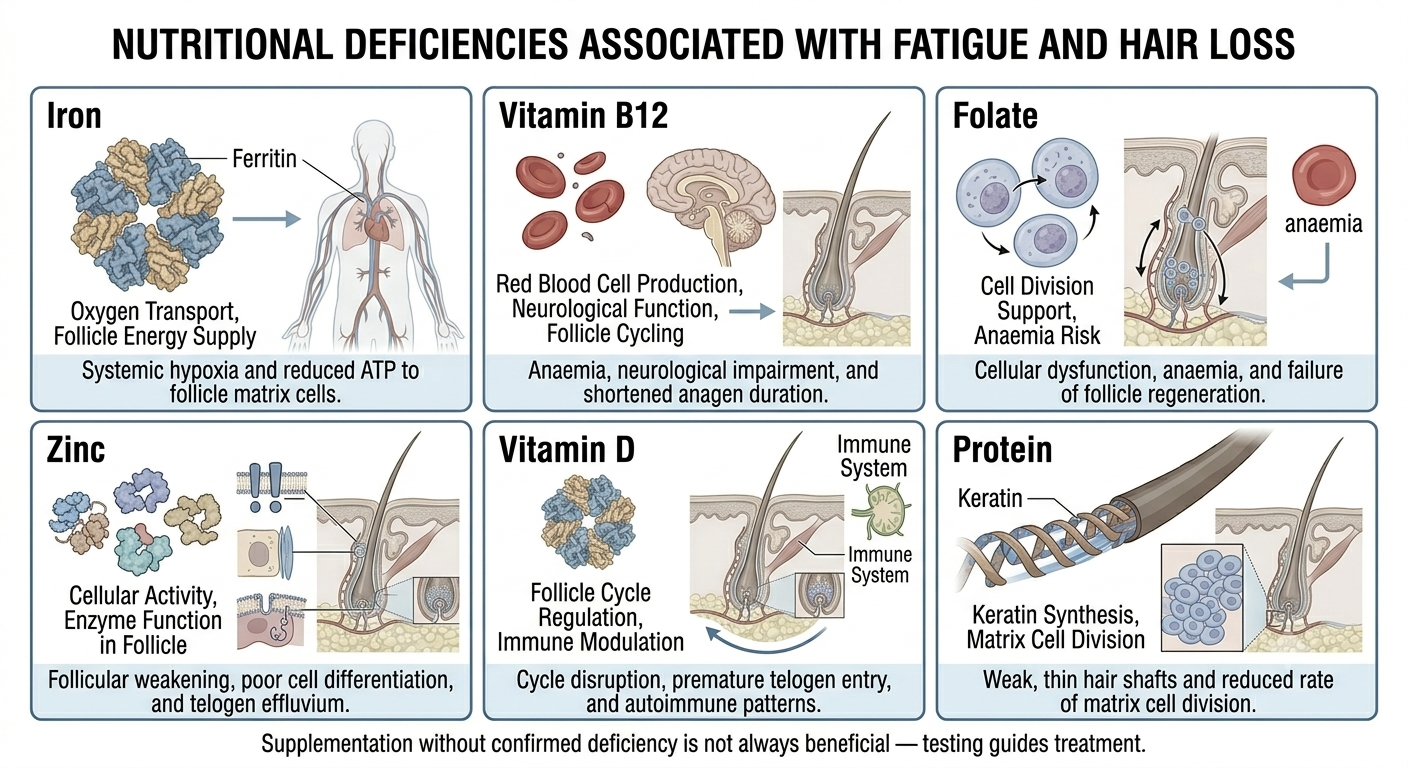
Nutritional deficiency goes beyond iron alone
Hair follicles require adequate nutritional support to maintain normal cycling and fibre production.
Deficiencies potentially associated with both fatigue and hair problems include:
Protein deficiency
Zinc deficiency
Vitamin D deficiency
Vitamin B12 deficiency
Folate deficiency
Severely restrictive diets, malabsorption disorders, eating disorders, and chronic gastrointestinal disease may all contribute.
However, supplementation without evidence of deficiency is not always helpful and sometimes creates unnecessary expense or side effects.
Chronic illness can present through the hair
Systemic diseases sometimes affect the hair before diagnosis.
Conditions potentially associated with fatigue and shedding include:
Autoimmune disease
Inflammatory bowel disease
Chronic infection
Kidney disease
Liver disease
Connective tissue disorders
Hair changes are usually not the only symptom, but they may form part of the broader clinical picture.
Persistent unexplained symptoms deserve proper medical assessment rather than assuming stress alone is responsible.
Autoimmune disease deserves consideration
Certain autoimmune disorders affect both energy levels and hair.
Examples include:
Lupus
Autoimmune thyroid disease
Alopecia areata
Coeliac disease
Inflammation, immune dysregulation, nutritional effects, and hormonal disruption may all contribute to fatigue and shedding patterns.
Autoimmune diseases often involve additional symptoms such as joint pain, rashes, digestive symptoms, or temperature sensitivity.
Post-viral shedding is increasingly recognised
After significant viral illness, some people experience prolonged fatigue followed by diffuse hair shedding.
This has been widely observed after severe influenza, COVID-19, and other systemic infections.
The mechanism is thought to involve physiological stress triggering telogen effluvium rather than direct destruction of follicles.
Hair usually regrows gradually over time, although recovery can feel slow and emotionally distressing.
Stress can affect both symptoms simultaneously
Psychological stress is sometimes dismissed too casually, but severe or chronic stress can genuinely influence both fatigue and hair cycling.
Stress may contribute to:
Sleep disruption
Hormonal changes
Altered eating patterns
Inflammatory signalling
Telogen effluvium
At the same time, not all fatigue and hair loss should automatically be blamed on stress. Medical causes should not be overlooked simply because someone appears anxious or busy.
Sleep disorders can indirectly contribute
Poor sleep quality affects the body broadly.
Conditions such as obstructive sleep apnoea may lead to:
Daytime exhaustion
Hormonal disruption
Inflammatory stress
Indirect effects on hair health may occur through broader metabolic strain rather than a direct follicle-specific mechanism.
People sometimes focus entirely on cosmetic treatment while missing severe chronic sleep deprivation.
Medications may contribute to both fatigue and shedding
Some medications are associated with diffuse hair shedding and reduced energy levels.
Examples may include certain:
Antidepressants
Blood pressure medications
Hormonal therapies
Anticoagulants
Retinoids
Anticonvulsants
Medication-related hair loss often presents as telogen effluvium rather than patchy baldness.
Reviewing medication history is therefore important during assessment.
Sudden severe fatigue deserves prompt attention
Certain symptom combinations require more urgent medical review.
Examples include fatigue with:
Rapid unexplained weight loss
Fever
Night sweats
Chest pain
Shortness of breath
Neurological symptoms
Heavy bleeding
Hair loss itself is rarely dangerous, but the associated systemic symptoms may be clinically important.
Hair texture changes can offer clues
Not only shedding but also texture changes sometimes accompany systemic disease.
Hair may become:
Dry
Coarse
Fragile
Sparse
Easily broken
These changes are not specific to one disease, but they may reinforce the need for broader evaluation.
Chronic dieting may destabilise hair growth
Aggressive calorie restriction places physiological stress on the body.
Rapid weight loss and inadequate protein intake are common triggers for telogen effluvium. People may feel fatigued while simultaneously experiencing diffuse shedding several months later.
This pattern is especially common after:
Crash dieting
Bariatric surgery
Extreme fitness programmes
Disordered eating
Recovery often depends on nutritional stabilisation and time.
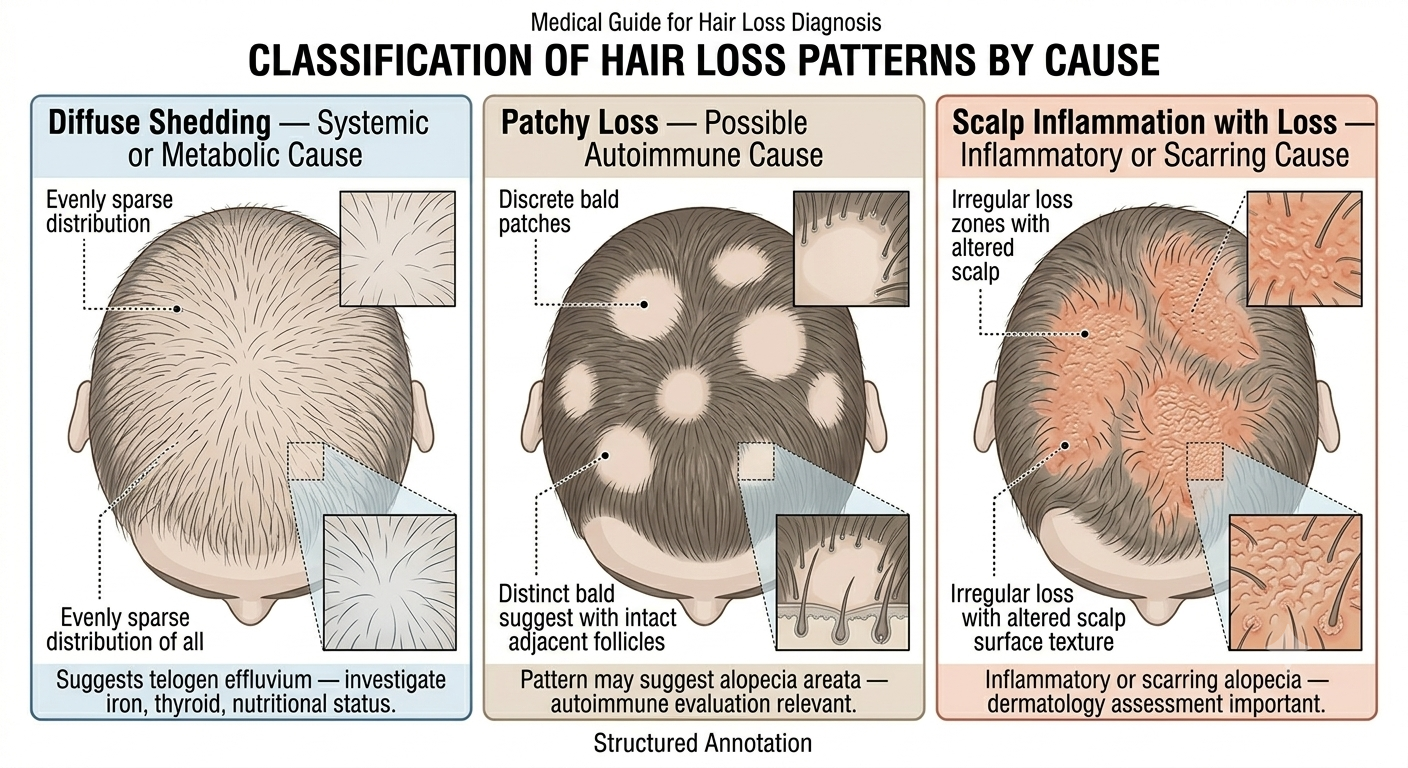
Hair loss patterns still matter diagnostically
Not all shedding with fatigue reflects the same process.
Diffuse shedding often suggests systemic or metabolic causes. Patchy hair loss may point more toward autoimmune disease such as alopecia areata. Scarring or inflammatory changes may indicate entirely different disorders.
The appearance of the scalp still provides important clinical information.
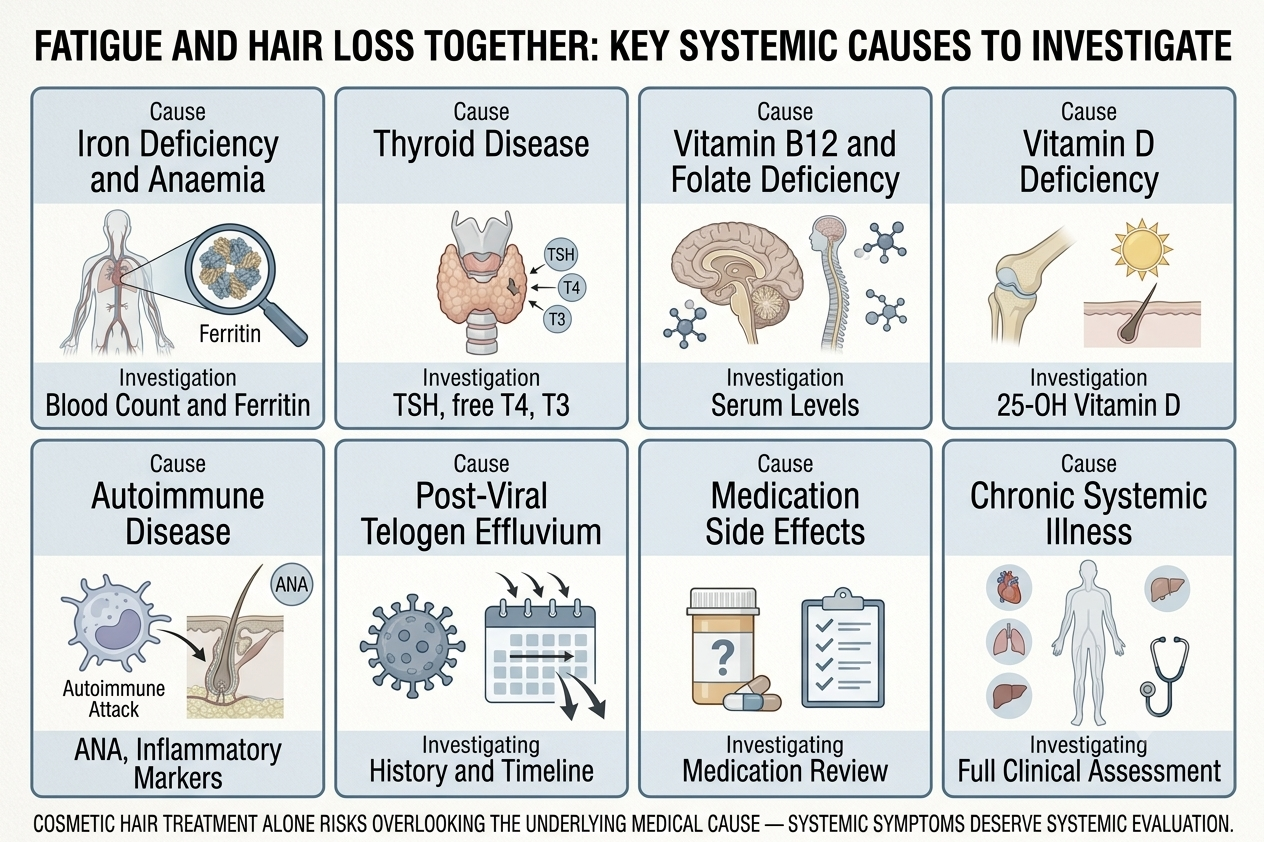
Blood testing is often part of assessment
Depending on symptoms and examination findings, clinicians may investigate:
Iron studies
Ferritin
Thyroid function
Vitamin B12
Vitamin D
Full blood count
Inflammatory markers
Testing varies according to the clinical picture rather than following a single universal checklist.
Cosmetic treatment alone may miss the real issue
Many people initially respond to hair loss by buying shampoos, oils, or supplements.
But if severe fatigue is present simultaneously, focusing only on cosmetic management risks overlooking an underlying medical condition.
Hair follicles sometimes act as early indicators of broader physiological stress.
The bottom line
Hair loss together with extreme fatigue deserves careful attention because the combination may reflect systemic disruption rather than an isolated scalp problem. Iron deficiency, anaemia, thyroid disease, nutritional deficiency, autoimmune conditions, chronic illness, major stress, and post-viral states are among the possibilities clinicians commonly investigate.
In many cases, the hair loss itself represents telogen effluvium triggered by internal stress affecting the body as a whole. Identifying and treating the underlying cause is usually far more important than relying solely on cosmetic hair products.
When fatigue is persistent, severe, or accompanied by additional symptoms, proper medical evaluation matters.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.
Add Comment