Hair thinning at the front of the scalp is often especially distressing for women because it directly affects framing of the face and can become difficult to conceal. Unlike diffuse thinning that develops gradually across the scalp, frontal hair loss tends to feel more visible and emotionally confronting early on.
But “front hair loss” is not a single diagnosis.
Several different medical conditions can affect the frontal scalp, and distinguishing between them matters because some are temporary, some progressive, and some potentially permanent if untreated.
The pattern itself often provides important diagnostic clues. A slowly widening part line behaves differently from recession at the temples. Patchy frontal loss differs from inflammatory thinning around the hairline.
This is one reason proper clinical assessment matters more than relying on general hair growth products alone.
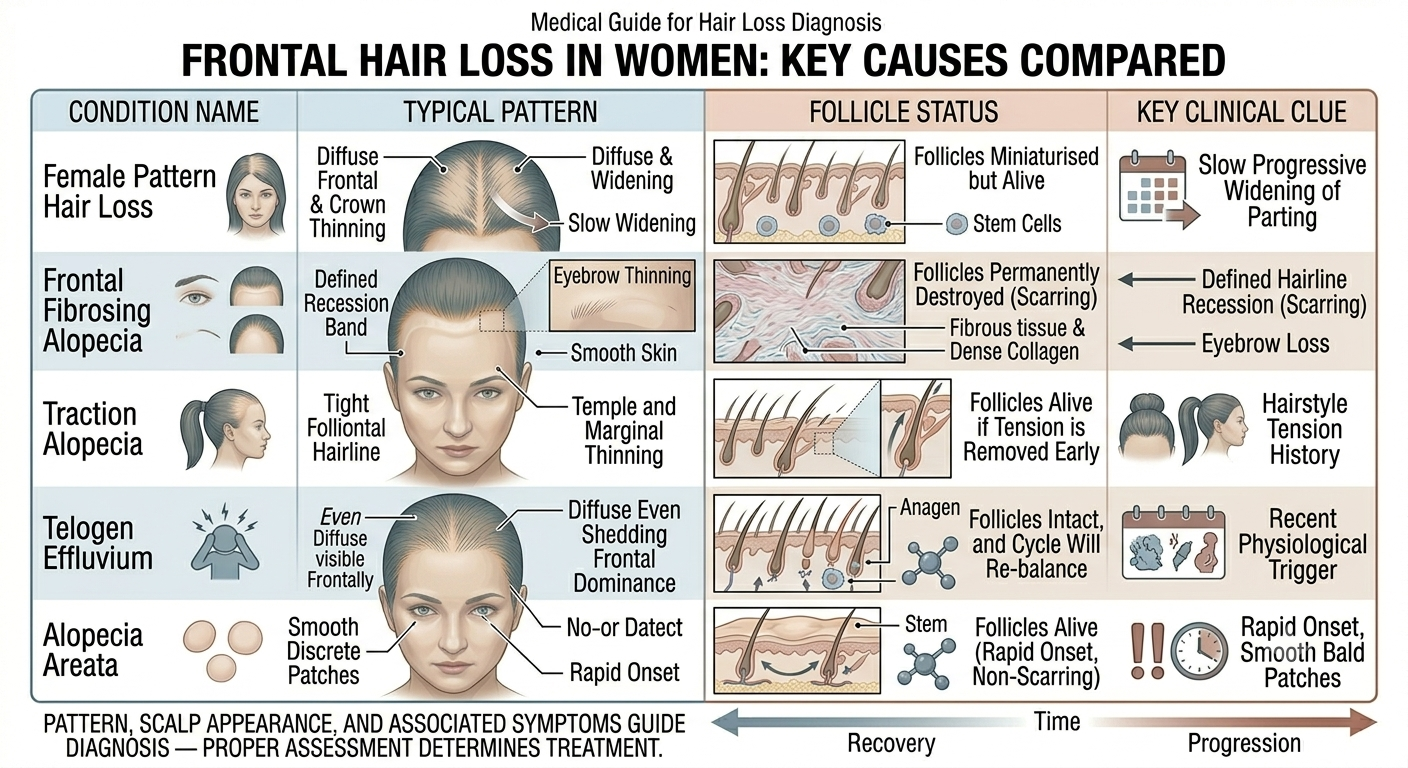
Female pattern hair loss can involve the frontal scalp
Female pattern hair loss, also called androgenetic alopecia, is one of the most common causes of frontal thinning in women.
Classically, women develop diffuse thinning over the crown while largely preserving the frontal hairline. However, this pattern is not universal.
Some women experience:
Reduced density near the front
Visible scalp through the frontal hairline
Temple thinning
Progressive widening of the part
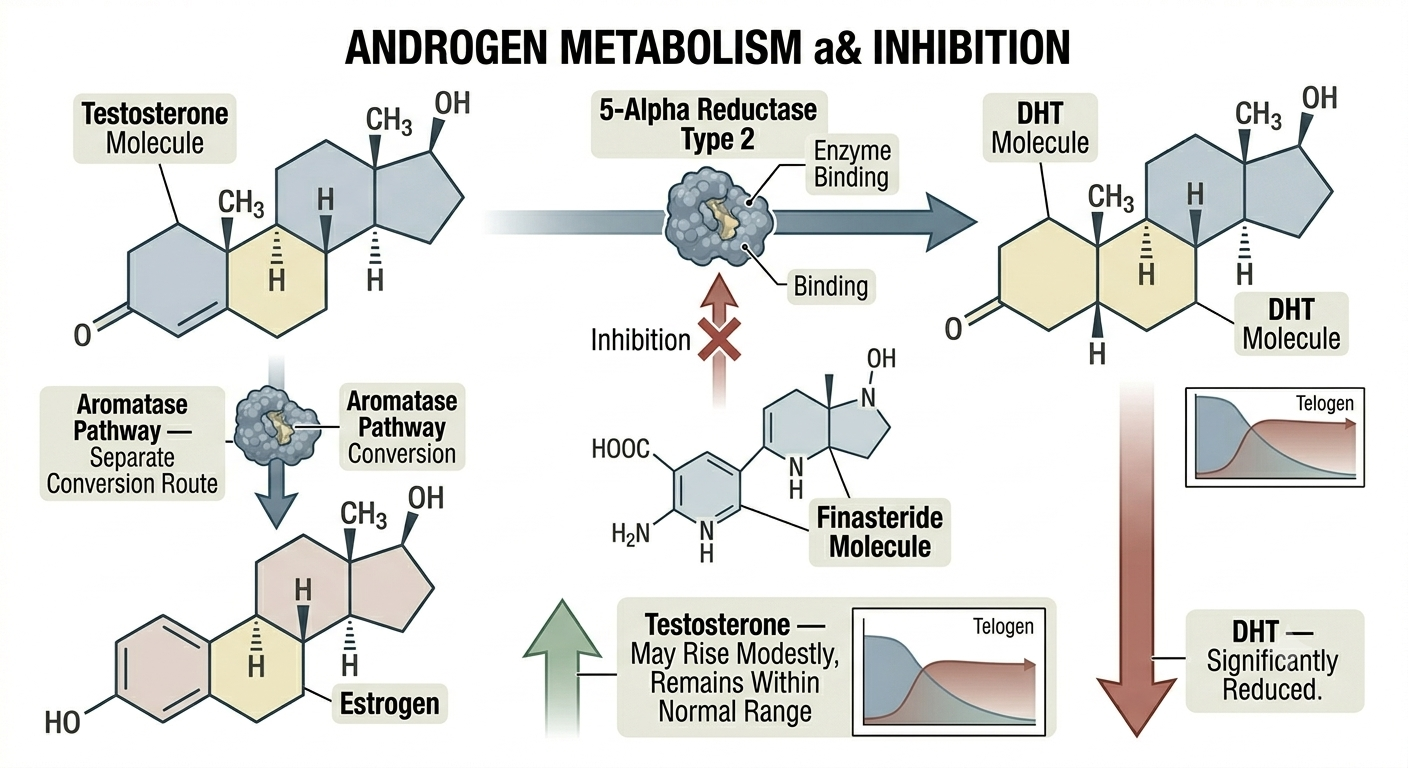
The condition involves gradual follicle miniaturisation influenced by genetics and hormonal sensitivity.
Unlike sudden shedding disorders, progression is usually slow and chronic.
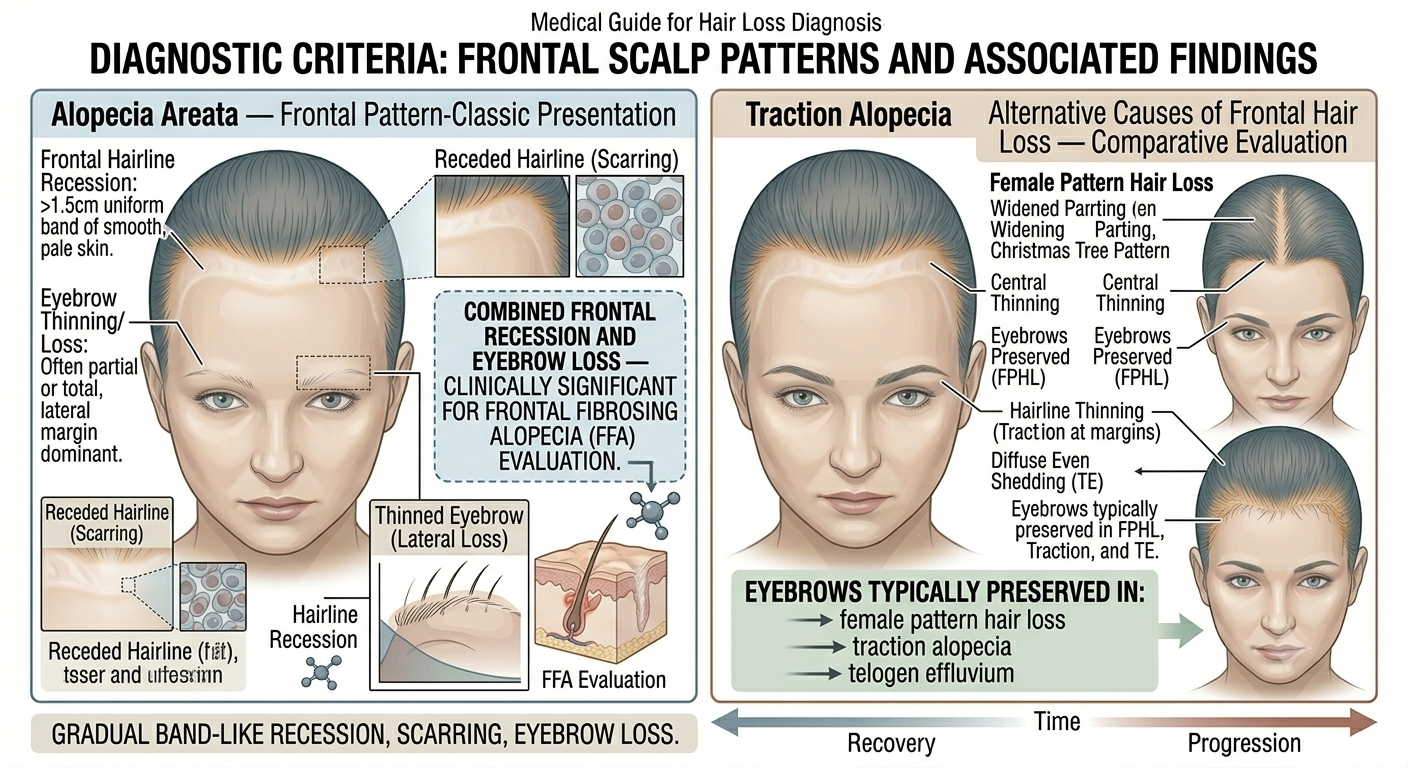
Frontal fibrosing alopecia is increasingly recognised
One important cause of frontal hairline loss in women is frontal fibrosing alopecia, or FFA.
FFA is a form of scarring alopecia in which inflammation gradually destroys follicles along the frontal hairline. It most commonly affects postmenopausal women, although younger women may also develop it.
Typical features include:
A receding frontal hairline
Loss of eyebrow hair
Smooth pale skin where follicles disappear
Scalp redness or irritation in some cases
Because follicle destruction may become permanent, early diagnosis matters.
Traction alopecia commonly affects the front and temples
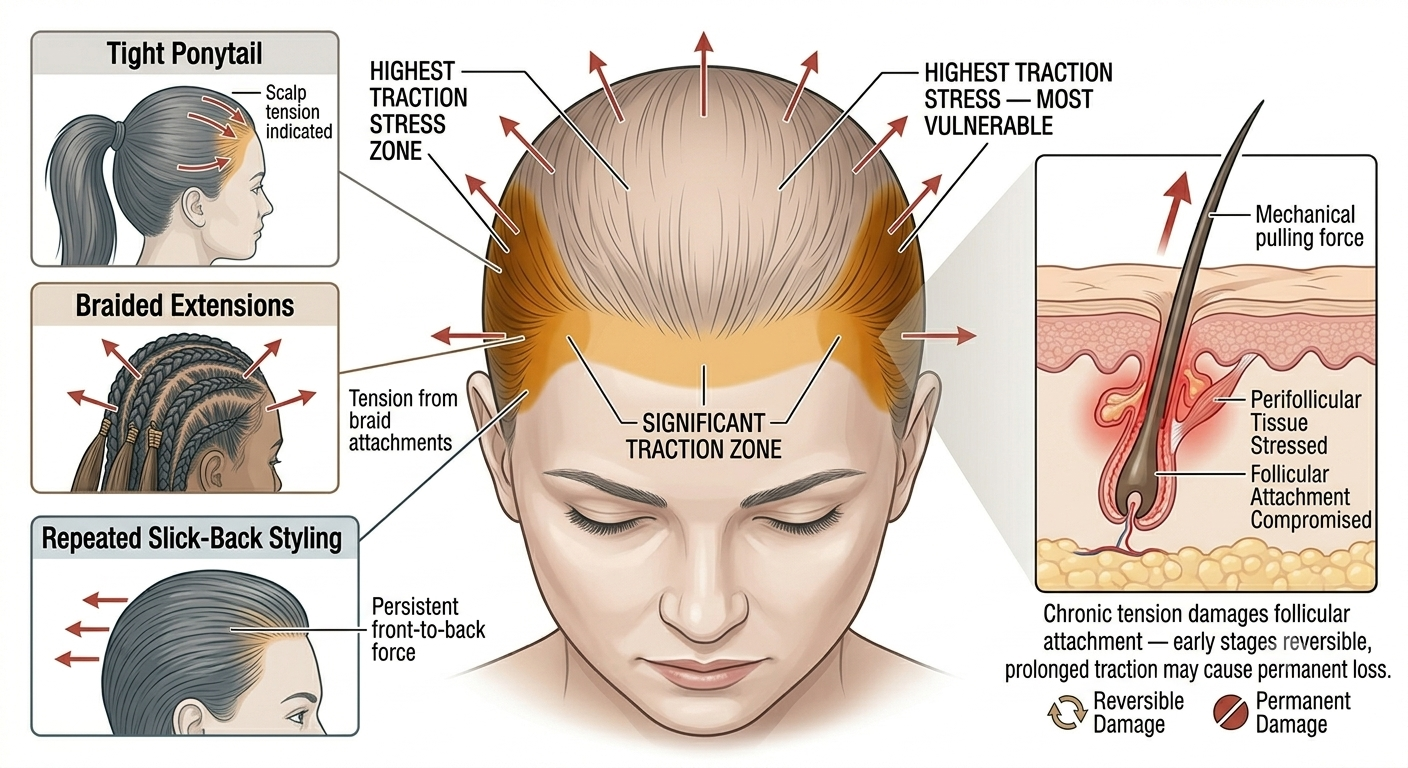
Traction alopecia develops from chronic tension on the hair.
The frontal scalp and temples are especially vulnerable because these areas often experience the greatest pulling forces during styling.
Risk factors include:
Tight ponytails
Braids under tension
Extensions
Repeated slick-back hairstyles
Heavy weaves
Initially, follicles may recover if tension stops. Longstanding traction, however, can eventually lead to permanent follicular damage.
Hormonal changes may alter the frontal hairline
Hormonal fluctuations influence follicle behaviour throughout the scalp.
Changes associated with:
Menopause
Polycystic ovary syndrome
Stopping hormonal contraception
Postpartum hormonal shifts
may all contribute to visible frontal thinning in susceptible women.
Hormonal effects are rarely the only factor involved, but they may accelerate genetically driven thinning patterns.
Thyroid disease can contribute to diffuse frontal thinning
Thyroid dysfunction often affects the hair diffusely, but frontal thinning may become particularly noticeable because facial framing changes quickly.
Hypothyroidism may cause:
Diffuse thinning
Dry coarse hair
Reduced hair density
Loss of the outer eyebrows
Hyperthyroidism may also trigger increased shedding.
Because thyroid disorders are relatively common and treatable, they are often investigated in women with unexplained hair changes.
Chronic telogen effluvium can make the front appear sparse
Telogen effluvium is a shedding disorder in which many follicles enter the resting phase prematurely.
Although shedding occurs diffusely, women often first notice reduced density at the front because this region is highly visible and receives strong lighting exposure.
Triggers may include:
Stress
Illness
Nutritional deficiency
Weight loss
Surgery
Major hormonal changes
Unlike scarring alopecia, follicles remain alive.
Hairline recession is not always androgen-driven
People often assume frontal recession automatically means androgenetic alopecia.
In women, however, frontal hairline changes may stem from:
Inflammation
Mechanical tension
Autoimmune disease
Scarring disorders
The pattern and scalp appearance help differentiate these conditions.
This is why examining the skin itself matters rather than focusing only on hair density.
Autoimmune conditions may affect the frontal scalp
Alopecia areata occasionally affects the frontal hairline.
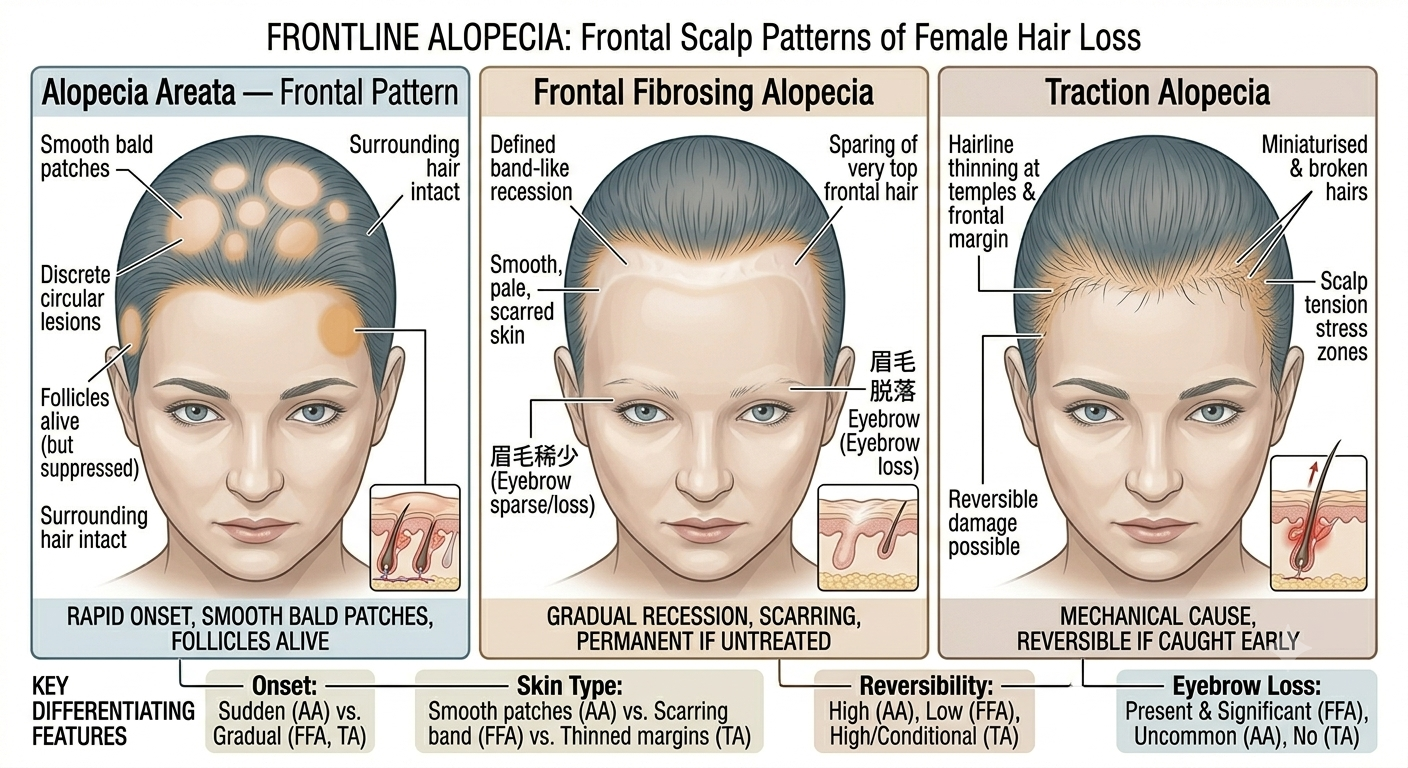
This autoimmune condition typically causes smooth round patches of sudden hair loss, but patterns vary considerably.
Some women develop band-like frontal involvement or patchy temple thinning that may initially resemble traction or pattern hair loss.
Rapid onset often provides an important clue.
Cosmetic practices can worsen fragility
Women trying to conceal frontal thinning sometimes unintentionally worsen breakage through repeated styling stress.
Contributing factors may include:
Heat styling
Frequent colouring
Aggressive brushing
Hair fibres applied heavily to the hairline
Tight camouflage styles
Breakage at the front may overlap with true follicular thinning, making the appearance seem worse.
Menopause changes the hormonal environment
After menopause, declining oestrogen levels alter the hormonal balance affecting follicles.
Some women notice:
Reduced density
Frontal thinning
Shorter hair growth cycles
Decreased strand diameter
At the same time, androgen-sensitive facial hair may increase.
These changes reflect complex hormonal shifts rather than a single isolated process.
Nutritional deficiency may contribute
Iron deficiency, severe calorie restriction, protein deficiency, and certain vitamin deficiencies may all contribute to increased shedding.
Again, frontal thinning may simply become the most visible area first.
Hair follicles are metabolically active and sensitive to systemic stress.
Frontal scalp inflammation should not be ignored
Symptoms such as:
Burning
Itching
Tenderness
Scaling
Redness
suggest possible inflammatory disease rather than purely cosmetic thinning.
Inflammatory conditions affecting the frontal scalp deserve proper dermatological evaluation because some forms can scar permanently if untreated.
Eyebrow loss may provide an important clue
When frontal thinning occurs together with eyebrow loss, doctors often consider frontal fibrosing alopecia among the possibilities.
This combination is clinically significant because eyebrow involvement is less typical in ordinary female pattern hair loss.
Associated facial papules or scalp discomfort may further support inflammatory disease.
Temple thinning is common but non-specific
Temple recession occurs in several conditions including:
Traction alopecia
Female pattern hair loss
Telogen effluvium
Scarring alopecia
The pattern alone rarely provides a complete diagnosis.
Clinical history and scalp examination remain important.
Stress alone is not always the answer
Women experiencing frontal hair loss are sometimes told the problem is “just stress” without proper assessment.
Stress certainly can contribute to shedding. But persistent frontal recession, inflammatory symptoms, or progressive thinning deserve careful evaluation rather than dismissal.
Several medically important conditions can mimic ordinary stress-related hair loss initially.
Dermoscopy often improves diagnostic accuracy
Hair specialists frequently use dermoscopy or trichoscopy to examine the scalp under magnification.
This helps identify:
Miniaturised hairs
Follicular inflammation
Loss of follicular openings
Scarring changes
Broken hairs
These details often clarify the diagnosis considerably.
Early treatment may preserve follicles
In non-scarring conditions, treatment aims to stabilise follicle cycling and reduce ongoing miniaturisation or shedding.
In scarring disorders, the priority becomes controlling inflammation before permanent destruction progresses further.
The earlier appropriate treatment begins, the greater the likelihood of preserving existing hair.
Cosmetic concealment remains reasonable
Medical treatment and cosmetic management are not mutually exclusive.
Many women use:
Strategic hairstyles
Hair fibres
Tinted powders
Volumising cuts
while medical evaluation and treatment continue.
These approaches may improve confidence without interfering with diagnosis.
The bottom line
Frontal hair loss in women has many possible causes including female pattern hair loss, traction alopecia, telogen effluvium, thyroid disease, autoimmune disorders, and scarring conditions such as frontal fibrosing alopecia.
Because some causes are reversible while others may lead to permanent follicle loss, proper diagnosis matters. The appearance of the hairline, associated symptoms, eyebrow involvement, scalp inflammation, and progression pattern all help doctors determine the underlying condition.
Front hair thinning is therefore not simply a cosmetic issue but sometimes an important clinical sign requiring medical assessment.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.


Add Comment