Hair does not grow continuously in a simple straight line. Every follicle on the scalp cycles through repeating biological phases of growth, transition, rest, and shedding.
These cycles are central to understanding nearly every major hair condition, from normal shedding to androgenetic alopecia, telogen effluvium, and post-illness hair loss.
People often panic when they see hairs falling out because they assume any shedding means something is wrong. In reality, some shedding is completely normal. Hair follicles are designed to release old hairs as part of their cycle.
Problems develop when the balance between these phases changes.
Understanding the hair cycle helps explain why hair loss can appear suddenly, why regrowth takes so long, and why many treatments require months before results become visible.
The hair follicle is biologically active
Hair follicles are not passive structures sitting in the scalp. They are highly active mini-organs with their own growth rhythms.
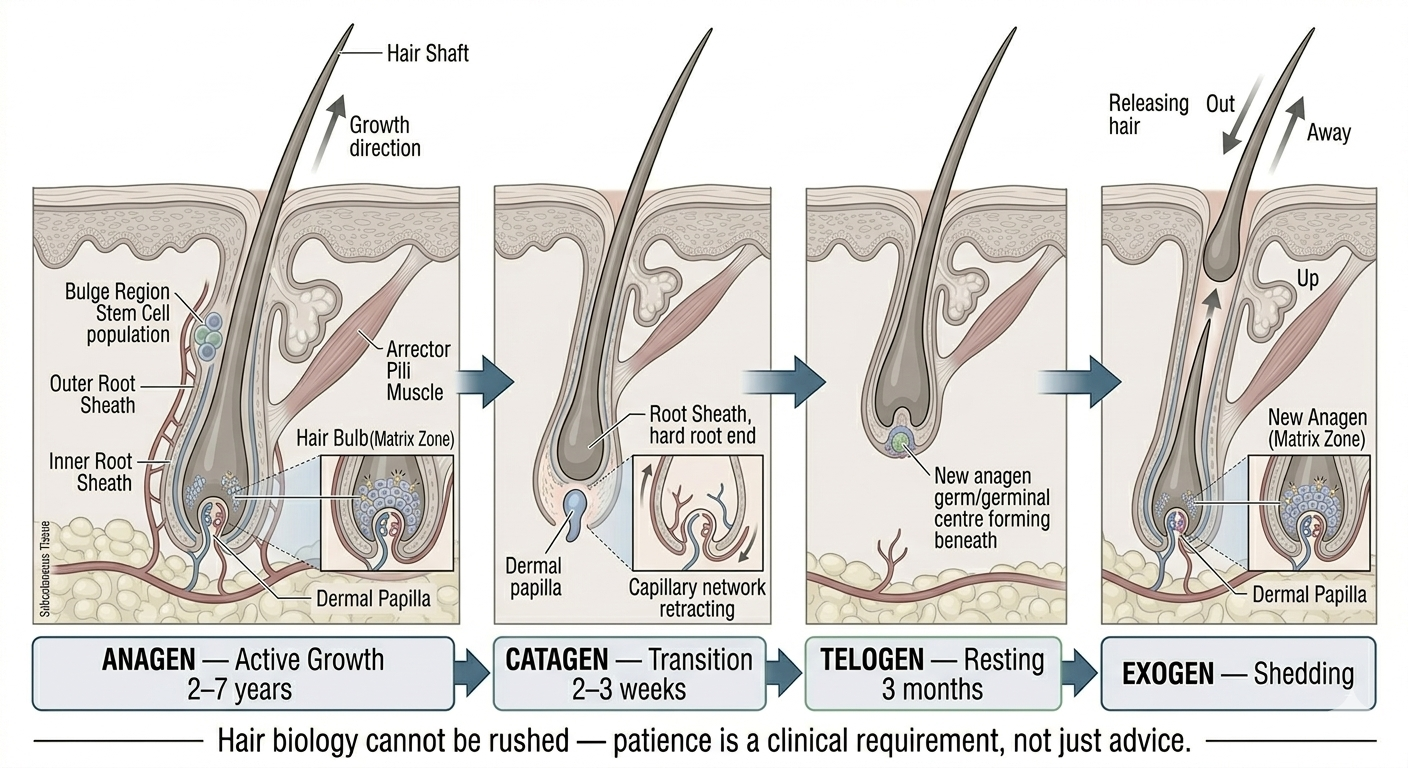
Each follicle independently cycles through phases:
Anagen
Catagen
Telogen
Some experts also describe a fourth phase called exogen, referring to the actual shedding process.
At any given moment, different follicles are in different stages. This is important because it prevents all scalp hair from shedding at once.
Anagen is the active growth phase
Anagen is the longest and most important stage for visible hair growth.
During anagen, the follicle actively produces the hair shaft. Cells divide rapidly at the root, pushing the hair upward and outward over time.
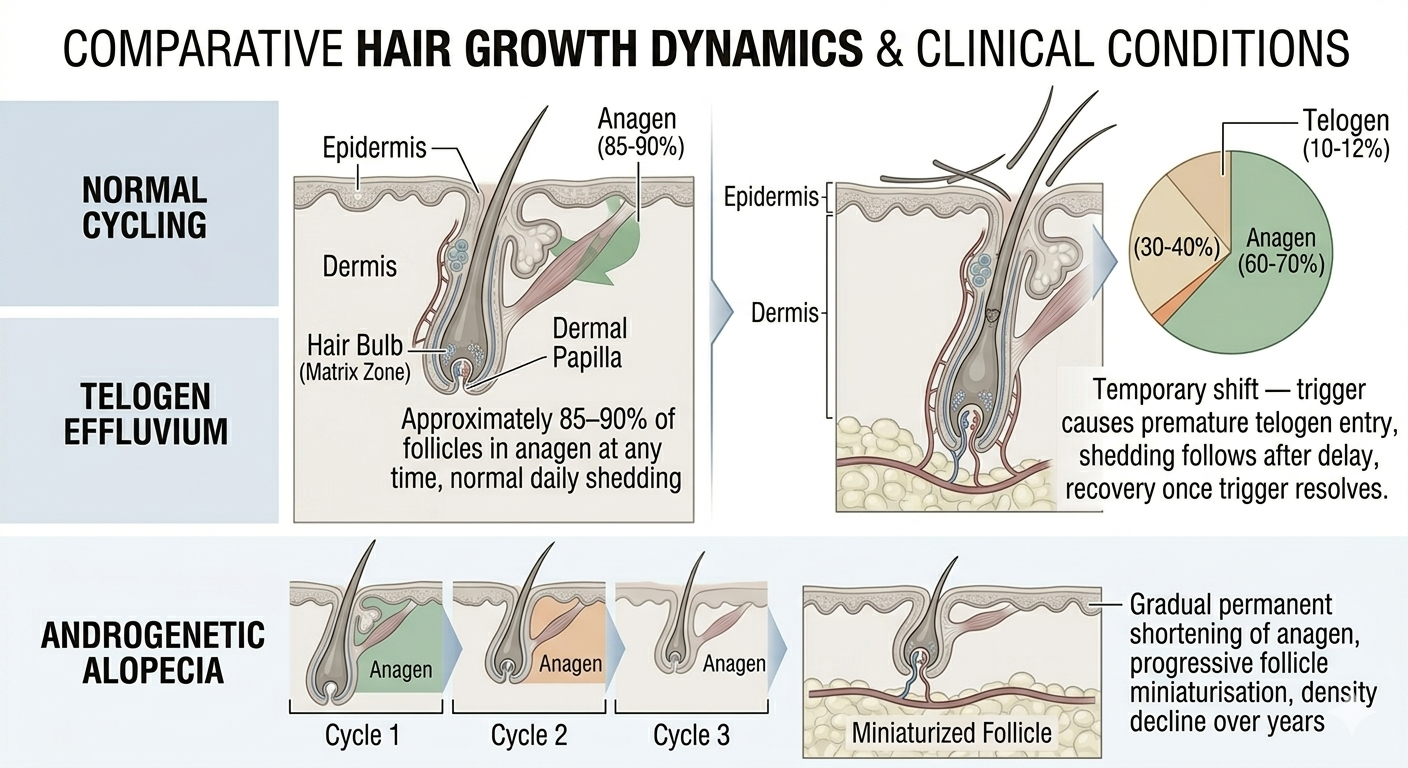
On a healthy scalp, most follicles are normally in anagen at any given moment.
The duration of anagen strongly influences maximum hair length. A person with a long anagen phase may grow very long hair naturally. Someone with a shorter anagen phase may find their hair reaches a certain length and seems to stop progressing.
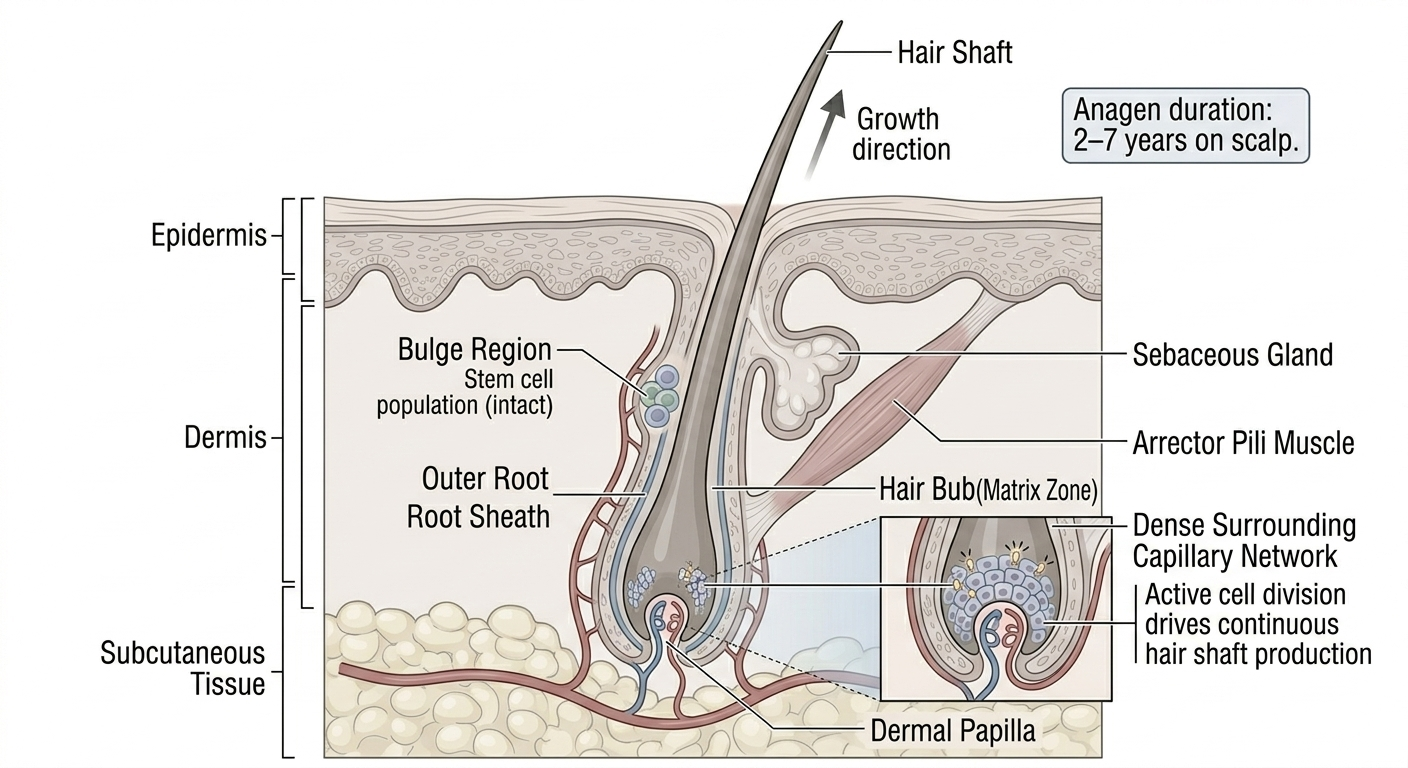
Scalp anagen can last several years.
Hair grows slowly even during anagen
One reason people become frustrated with hair treatments is that even active growth is relatively slow.
Human scalp hair typically grows around one to 1.25 centimetres per month on average, though individual variation exists.
This means visible changes take time.
Even when a treatment is working properly, the biology itself remains gradual.
Anagen duration affects density and fullness
Longer anagen phases generally support fuller-appearing hair because follicles spend more time actively producing strands.
Certain hair disorders shorten the anagen phase. When this happens, hairs may:
Grow for less time
Become shorter
Miniaturise
Shed earlier
This contributes to reduced density over time.
In androgenetic alopecia, for example, susceptible follicles gradually spend less time in anagen while producing finer hairs.
Catagen is the transition phase
Catagen is much shorter than anagen.
During this stage, active growth stops. The follicle begins shrinking and detaching from its deep blood supply.
This is a controlled biological transition rather than damage.
Catagen usually lasts only a few weeks.
Because it is relatively brief, only a small percentage of scalp follicles are normally in catagen at any moment.
Telogen is the resting phase
After catagen, the follicle enters telogen.
During telogen, the hair is no longer actively growing. The follicle rests while retaining the existing hair shaft temporarily.
Eventually, the old hair is released and a new cycle begins.
Telogen typically lasts a few months.
Again, this is normal biology. A certain proportion of hairs are always in telogen.
Shedding is part of the cycle
Normal scalp shedding happens because hairs completing telogen are released.
People naturally lose hairs during:
Brushing
Washing
Styling
Sleeping
The exact number varies considerably between individuals.
Many healthy people shed around 50 to 100 hairs daily without developing visible thinning.
The problem is not shedding alone. The problem is excessive shedding, poor regrowth, follicle miniaturisation, or changes in cycle balance.
Exogen refers to the shedding stage
Some specialists separately describe exogen as the phase where the old hair shaft exits the follicle.
This process overlaps with telogen and helps explain why hairs often come out during washing or brushing.
Importantly, shedding a hair does not mean the follicle itself is dead. In many cases, a new cycle is already beginning underneath.
Why telogen effluvium happens
Telogen effluvium is one of the clearest examples of disrupted hair cycling.
In this condition, a larger-than-normal number of follicles shift prematurely into telogen after a physiological stressor such as:
Illness
Surgery
High fever
Childbirth
Rapid weight loss
Nutritional deficiency
Psychological stress
Medication changes
Because telogen lasts several months, shedding usually begins well after the triggering event. This delay often confuses people.
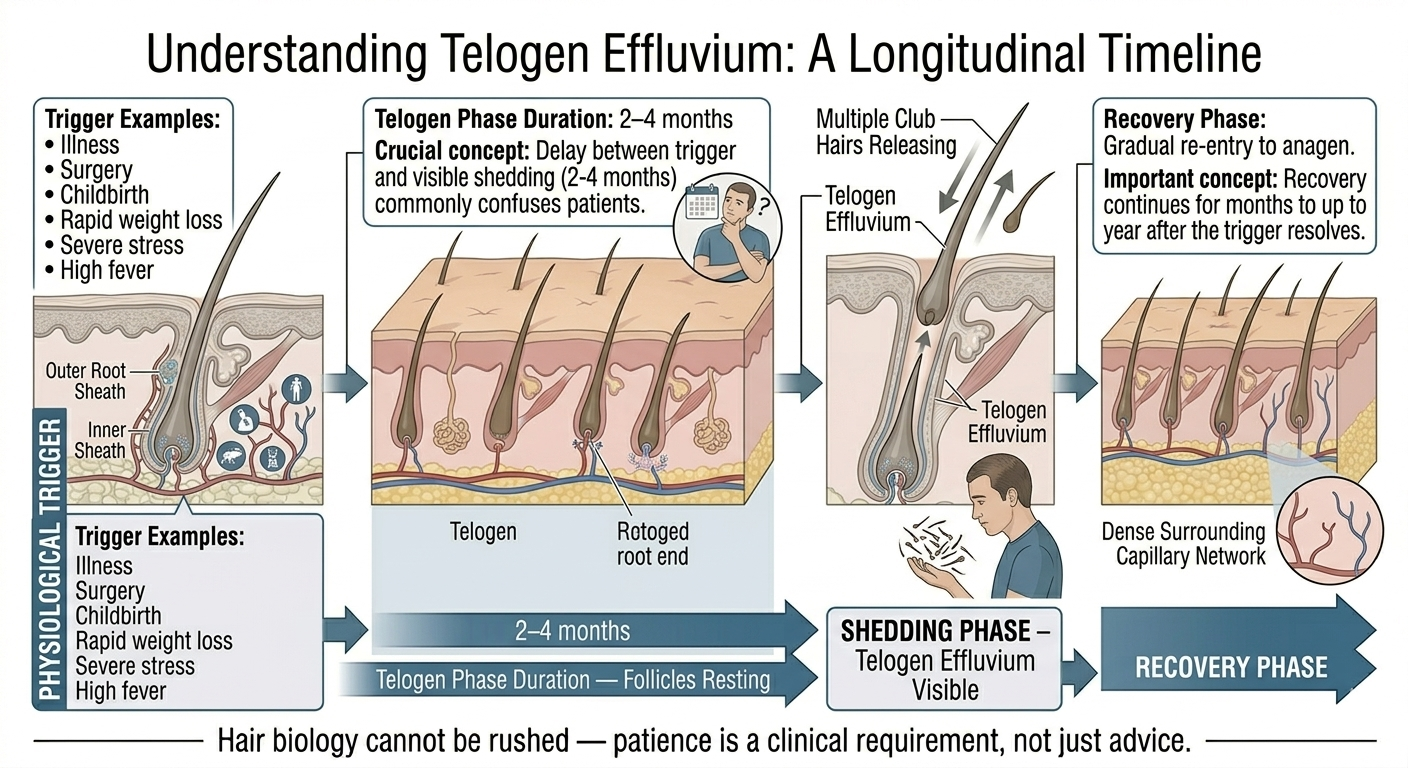
A person may become ill in January but only notice dramatic shedding in March or April.
Hair cycling explains delayed regrowth too
People recovering from telogen effluvium often expect immediate improvement once the trigger resolves.
But follicles still need time to cycle back into anagen and produce visible new hair.
This is why recovery may continue gradually for many months even after the underlying issue improves.
Hair biology works on delayed timelines.
Androgenetic alopecia changes the cycle progressively
Pattern hair loss affects follicle cycling in a different way.
In androgenetic alopecia, genetically susceptible follicles become increasingly sensitive to dihydrotestosterone, or DHT.
Over time:
Anagen shortens
Telogen proportion increases
Hairs miniaturise
Density declines
Eventually, follicles may produce very fine, short hairs that provide little cosmetic coverage.
This process usually occurs gradually rather than suddenly.
Treatments often aim to influence the cycle
Many hair loss treatments work partly by affecting hair cycling.
Minoxidil appears to prolong anagen in some follicles and may encourage resting follicles to re-enter active growth.
Finasteride reduces DHT-related miniaturisation, helping preserve healthier cycling patterns in susceptible follicles.
Other treatments attempt to support follicle function indirectly through different mechanisms, though evidence quality varies considerably.
Initial shedding during treatment can happen
One confusing aspect of treatment is temporary increased shedding.
Some people starting minoxidil notice more shedding initially because follicles may synchronise into new growth cycles. Older telogen hairs are released while newer anagen hairs begin developing.
This can be emotionally difficult because patients fear the treatment is worsening hair loss.
Not every patient experiences this, and increased shedding does not automatically mean the treatment is working. But temporary cycle shifts can occur.
Hair cycles vary between body areas
Not all hair behaves like scalp hair.
Eyebrows, eyelashes, beard hair, body hair, and scalp hair all have different cycle durations.
Scalp follicles have particularly long anagen phases compared with many other body areas. This is one reason scalp hair can grow to substantial lengths while eyebrow hairs remain relatively short.
Hormones also influence these cycles differently depending on body region.
Age affects the cycle
Hair cycling changes with age.
Older individuals may experience:
Shorter anagen duration
Reduced density
Finer hairs
Slower recovery after shedding events
Hair may therefore appear thinner even without dramatic disease processes.
Ageing follicles often produce less robust hair over time.
Inflammation can disrupt cycling too
Inflammatory scalp conditions may interfere with normal follicle behaviour.
Conditions such as:
Seborrhoeic dermatitis
Psoriasis
Scarring alopecias
Severe folliculitis
can alter the scalp environment and potentially affect growth cycling.
Scarring alopecias are particularly important because inflammation may permanently damage follicles if untreated.
Hair cycle timing explains why patience matters
People frequently abandon treatments too early because they expect rapid visible changes.
But follicles need time to:
Exit resting phases
Re-enter growth
Produce measurable length
Improve density visibly
Even effective therapies often require at least several months before meaningful evaluation is possible.
Hair biology cannot be rushed dramatically.
Seasonal shedding may occur
Some research suggests mild seasonal variation in hair cycling, though this area remains incompletely understood.
Some individuals report increased shedding during certain times of year, particularly autumn.
These changes are usually temporary and mild compared with pathological shedding disorders.
When hair cycling deserves medical evaluation
Cycle disruption may warrant medical assessment when shedding is:
Sudden
Severe
Patchy
Associated with scalp symptoms
Accompanied by fatigue or systemic symptoms
Progressively worsening
Hair cycle changes sometimes reflect broader medical conditions rather than isolated cosmetic concerns.
The bottom line
Hair follicles cycle continuously through phases of growth, transition, rest, and shedding. Anagen drives active growth, catagen marks transition, and telogen represents the resting stage before hairs are released.
These cycles explain why normal shedding occurs, why stress-related hair loss appears delayed, why pattern baldness develops gradually, and why hair treatments require patience.
Most importantly, hair loss is rarely random. Understanding follicle cycling helps make sense of the slow, often frustrating timelines involved in both shedding and recovery.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.
Add Comment